fetching data ... 
Background: ASCORE (Abatacept SubCutaneOus in Routine clinical practicE; NCT02090556) is an ongoing, prospective, non-interventional, multicentre study of patients (pts) with RA receiving SC abatacept (ABA). In a similar real-world setting, IV ABA retention was >88% at 6 months (M).1
Objectives: To present baseline (BL) pt characteristics and 6M interim retention rates and clinical outcomes for SC ABA by biologic (b)DMARD treatment line.
Methods: Pts (≥18 years) with active, moderate-to-severe RA, naïve to ABA and who initiated SC ABA 125 mg weekly were enrolled across 10 countries (March 2013–January 2017) in 2 cohorts: biologic-naïve pts and pts who had failed ≥1 prior bDMARD. In some countries, an IV loading dose was administered according to local practice. Pt demographics and disease characteristics at SC ABA initiation were recorded. The retention rate (95% CI) of SC ABA over 6M was estimated by Kaplan–Meier analysis. Good/moderate EULAR response rates based on DAS28 (ESR, otherwise CRP), low disease activity (LDA) or remission according to DAS28 (ESR), CDAI, SDAI and Boolean criteria were assessed at 6M.
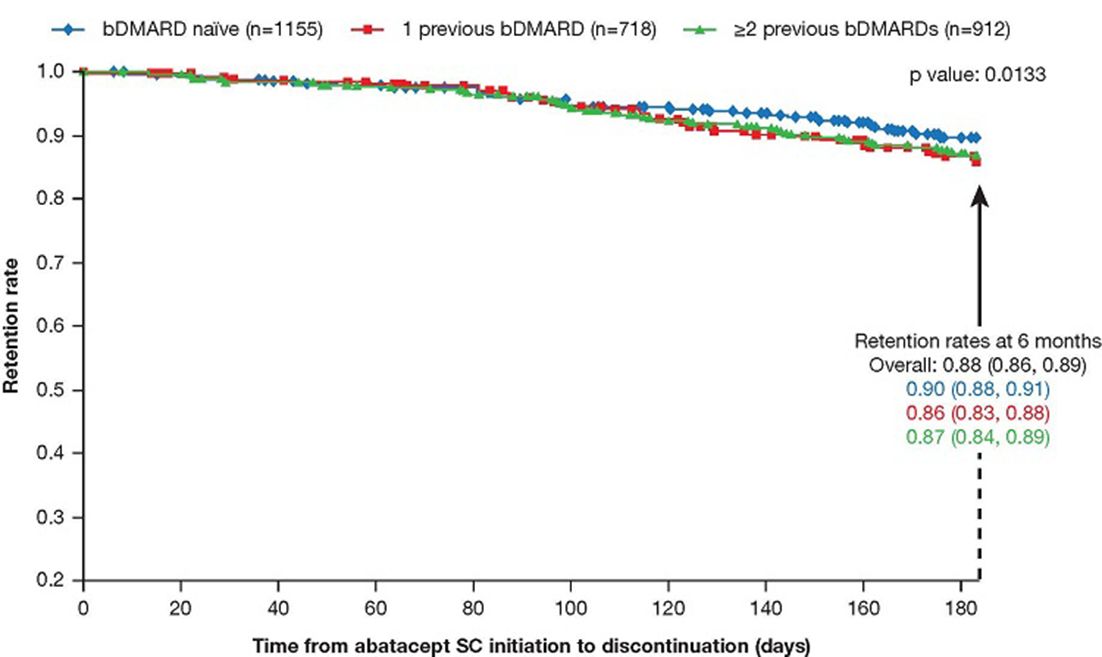
Results: Of 2943 pts enrolled, 2785 (94.6%) were evaluable: 1155 (41.5%) biologic naïve; 718 (25.8%) had failed 1; and 912 (32.7%) had failed ≥2 prior biologics. At BL, there was a higher proportion of females and pts with longer disease duration among those who had failed ≥2 vs 1 or no prior bDMARDs; disease activity was similar across treatment lines; CRP was higher in biologic-naïve vs -failure pts; 402 (48.4%) biologic-naïve pts had erosive disease vs 261 (53.7%) or 390 (63.8%) who had received 1 or ≥2 prior bDMARDs, respectively. Probability of overall SC ABA retention at 6M was 0.88 (95% CI 0.86, 0.89); retention was higher in pts receiving ABA as a first or second vs later bDMARD (figure 1). At 6M, 335 pts had discontinued ABA, 172 (51.3%) of whom due to inefficacy and 140 (41.8%) due to safety. At 6M, among pts continuing ABA, good/moderate EULAR response rates were 83.5%, 75.1% and 72.0% for biologic-naïve pts and pts with 1 and ≥2 prior bDMARD failures, respectively. DAS28 (ESR), CDAI or SDAI LDA/remission, or Boolean remission rates were higher with earlier vs later treatment lines. The safety profile was consistent with IV ABA studies.1,2
Abstract AB0461 – Figure 1 Abatacept Retention (Time to Discontinuation of SC Abatacept) Over 6 Months by Treatment Line
Conclusions: In this first observation of SC abatacept in a real-world setting, overall retention of SC abatacept at 6M was high and similar to that observed with IV abatacept.1 Better retention and response rates were achieved with abatacept as an earlier bDMARD treatment line. Good/moderate EULAR response rates at 6M were consistently >70%, irrespective of treatment line and higher BL radiographic erosion in biologic-failure pts.
References:
Disclosure of Interest: R. Alten Grant/research support from: Bristol-Myers Squibb, Speakers bureau: Bristol-Myers Squibb, X. Mariette Grant/research support from: Biogen, Pfizer, UCB, Speakers bureau: Bristol-Myers Squibb, LFB, GSK, Pfizer, UCB, M. Buch Grant/research support from: AbbVie, AstraZeneca, Eli Lilly, Pfizer, Roche, Sandoz, UCB, Consultant for: AbbVie, AstraZeneca, Eli Lilly, Pfizer, Roche, Sandoz, UCB, R. Caporali Speakers bureau: Bristol-Myers Squibb, AbbVie, Celgene, Eli Lilly, MSD, Pfizer, Roche, UCB, R.-M. Flipo Consultant for: Bristol-Myers Squibb, A. Forster Consultant for: AbbVie, Bristol-Myers Squibb, Pfizer, Celgene, Roche, Novartis, UCB Pharma, Speakers bureau: AbbVie, Bristol-Myers Squibb, Pfizer, Celgene, Roche, Novartis, UCB Pharma, H. Griffiths Grant/research support from: AbbVie, Janssen, and Sanofi, Consultant for: Bristol-Myers Squibb and Janssen, Paid instructor for: Novartis, M. Nurmohamed Grant/research support from: Pfizer, AbbVie, Roche, Bristol-Myers Squibb, MSD, Mundipharma, UCB, Janssen, Menarini, Eli Lilly, Sanofi, Celgene, Consultant for: Pfizer, AbbVie, Roche, Bristol-Myers Squibb, MSD, Mundipharma, UCB, Janssen, Menarini, Eli Lilly, Sanofi, Celgene, Speakers bureau: Pfizer, AbbVie, Roche, Bristol-Myers Squibb, MSD, Mundipharma, UCB, Janssen, Menarini, Eli Lilly, Sanofi, Celgene, Y. Patel Grant/research support from: Bristol-Myers Squibb, Pfizer, AbbVie, Speakers bureau: Bristol-Myers Squibb, Pfizer, AbbVie, P. Peichl Consultant for: Bristol-Myers Squibb, Eli Lilly, R. Sanmarti Grant/research support from: Bristol-Myers Squibb, Consultant for: Bristol-Myers Squibb, C. Chauvet Employee of: Bristol-Myers Squibb, J. Heitzman Employee of: Bristol-Myers Squibb, C. Rauch Employee of: Bristol-Myers Squibb, S. Connolly Employee of: Bristol-Myers Squibb
DOI: 10.1136/annrheumdis-2018-eular.1992