fetching data ... 
Background: In new-onset rheumatoid arthritis (RA), therapy should be aimed at achieving sustained remission according to current guidelines, in which methotrexate (MTX) is recommend to be included in the initial treatment strategy. However, a large proportion (~30%) eventually need additional treatment to control inflammation making it necessary to find predictors which helps clinicians in choosing the optimal initial therapy to further improve the long-term outcome of early RA patients.
Objectives: To identify and validate clinical baseline predictors associated with inadequate response (IR) to MTX therapy in disease modifying anti-rheumatic drug (DMARD)-naïve early RA patients.
Methods: For identifying clinical predictors, data was used from the U-Act-Early trial of newly diagnosed RA patients treated-to-target with a MTX strategy (n=108, development sample). MTX (oral) was started at 10 mg/week and increased in monthly steps up to 30 mg/week or maximum tolerable dose until remission. If no remission, hydroxychloroquine (HCQ) was added and, if the target, remission, thereafter still was not achieved, HCQ was replaced by tocilizumab. Patients in the tREACH trial who initiated MTX (25 mg/week) in combination with a prednisone tapering scheme were used as validation sample (n=83). In tREACH, if disease activity score (DAS) was ≥2.4 after three months, etanercept was added. When three months thereafter the target still was not achieved, patients switched to another tumour necrosis factor alpha inhibitor. In both studies, the definition of IR to MTX, (designated here “MTX+” therapy), was met if patients needed a biological DMARD within the first year. Clinical predictors were identified using logistic regression with backward selection (p≤0.10).
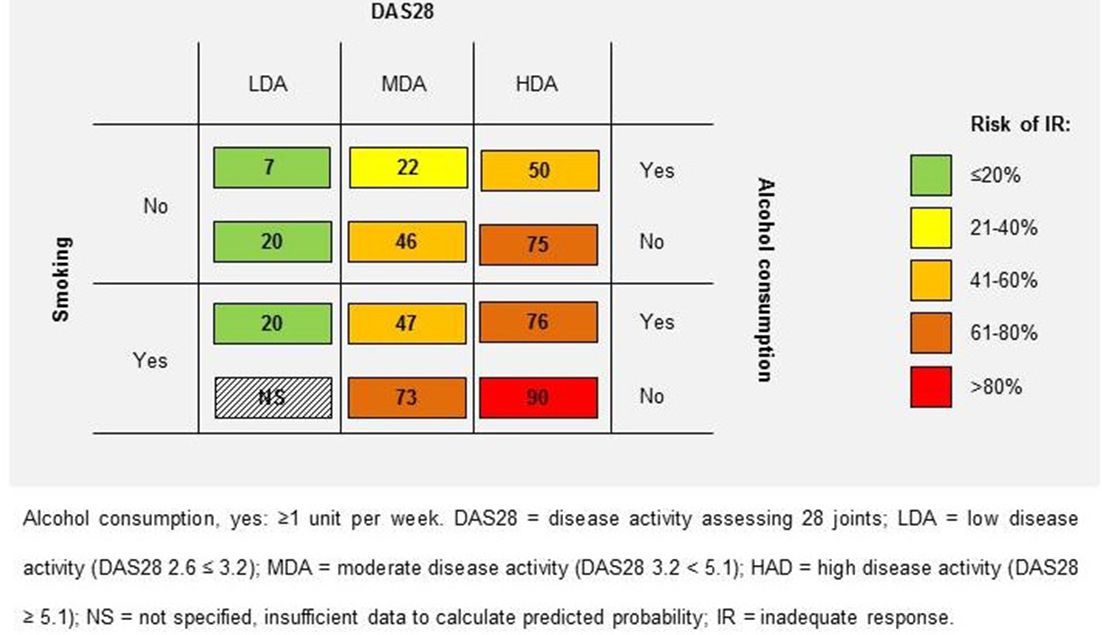
Results: In the development sample, the following predictors for IR to “MTX+” therapy were identified: DAS assessing 28 joints (DAS28), adjusted odds ratio (ORadj) 2.1, 95% CI 1.4–3.1; p<0.001; current smoking, ORadj 3.0, 95% CI 1.1–8.0; p=0.027; and alcohol consumption, ORadj 0.3, 95% CI 0.1–0.9; p=0.021. A risk matrix, categorised by these predictors, shows nearly a twelve and a halve fold risk difference in predicted probabilities (figure 1). The area under the receiver operating characteristic curve (AUROC) of the model is 0.75 (95% CI 0.66–0.84); no statistically significant difference (p=0.96) was found between the observed and predicted probabilities (i.e. calibration). When using a negative predictive value (NPV), i.e. predicted chance of not failing “MTX+” therapy, of >80% as cut off in the development sample, the positive predictive value (PPV) was 65% (sensitivity: 0.89, specificity: 0.52). The AUROC of the model in the validation sample was 0.67 (95% CI 0.55–0.79) with no significant difference (p=0.28) between observed and predicted probabilities, indicating good calibration. In the validation sample, a cut-off of NPV >80%, the PPV was 54% (sensitivity: 0.88, specificity: 0.38).
Abstract FRI0040 – Figure 1 Risk matrix of predicted probability (%) of IR to “MTX+” therapy.
Conclusions: Higher DAS28, current smoking and no alcohol consumption were associated with an increased risk of IR to “MTX+” therapy in newly diagnosed RA patients.
Disclosure of Interest: X. Teitsma: None declared, J. Jacobs Grant/research support from: The department of the author (JWGJ) who included patients in the U-Act-Early trial received reimbursements from Roche Nederland BV., P. Welsing: None declared, P. de Jong: None declared, J. Hazes: None declared, A. Weel: None declared, A. Pethö-Schramm Employee of: AP-S is an employee of F Hoffmann-La Roche, M. Borm Employee of: MEAB is an employee of Roche Nederland BV, J. van Laar Grant/research support from: JMvL received fees from Arthrogeen, MSD, Pfizer, Eli Lilly, and BMS and research grants from Astra Zeneca, Roche-Genentech., F. Lafeber Grant/research support from: FPJGL reports grants from Roche, J. Bijlsma Grant/research support from: JWJB reported grants and fees from Roche, AbbVie, Bristol-Myers Squibb, Merck Sharp and Dohme, Pfizer, and UCB
DOI: 10.1136/annrheumdis-2018-eular.3463