fetching data ... 
Background: Tenosynovitis (TSV) occurs in individuals at-risk of developing RA and could explain pain and stiffness in the absence of synovitis. TSV of the wrist and finger flexor tendons has been described in at-risk individuals but involvement of other hand tendons has not been well investigated. The hand interossei are crucial to hand function and can become inflamed in RA(.1 Whether the interosseous tendons (IT) are sites of inflammation in at-risk individuals, and how this relates to joint inflammation and clinical features is unknown.
Objectives: To describe the anatomy, prevalence, pattern and clinical associations of IT inflammation in anti-CCP positive at-risk individuals.
Methods: Anti-CCP positive individuals with no synovitis (CCP+), healthy controls (HC), DMARD-naïve early RA patients (ERA) and treated ‘late’ RA patients (LRA) were recruited. All subjects underwent clinical and MRI assessment. 1.5T or 3T unilateral hand MRI scans were consensus scored for RAMRIS, TSV and IT inflammation by two radiologists. IT inflammation was defined as enhancing tissue around the tendon evident in two planes. For RAMRIS and tenosynovitis, scores were adjusted for 193 age-matched controls(.2 To understand the anatomical basis for MRI IT inflammation, a cadaveric study was performed on 20 fresh hand specimens; coloured dyes were injected along the first dorsal IT and into the adjacent second MCP joint and specimens were frozen and sectioned.
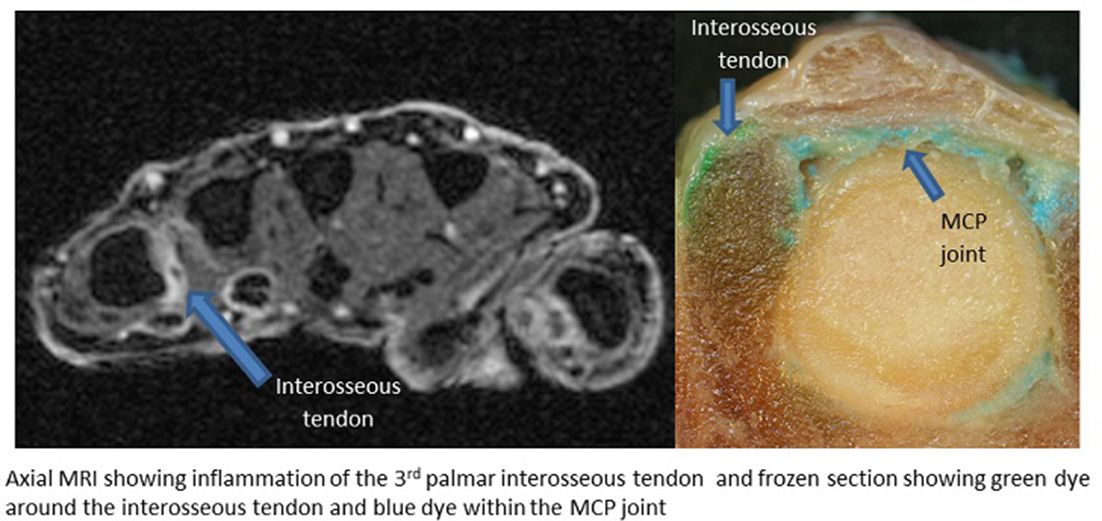
Results: 93 CCP+, 20 HC, 47 ERA and 28 LRA were recruited. Frequency of swollen and tender joints, MRI inflammation (synovitis, BME, erosions, TSV) and CRP level increased along the RA continuum with increasing disease duration. The proportion of patients with IT inflammation increased along the RA continuum. No HC, 18/93 (19%) CCP+, 23/47 (49%) ERA and 16/28 (57%) LRA patients had inflammation of ≥1 IT (p<0.001). The number of affected ITs increased along the RA continuum (p<0.001) and tendons associated with MCPJs 2 and 5 were most commonly affected. IT inflammation and MRI synovitis were associated with MCPJ swelling [OR 2.7 (0.9, 8.1) and OR 3.1 (1.0, 9.8) respectively] but IT inflammation was the only feature independently associated with MCPJ tenderness [OR 3.1 (1.4, 6.8) p=0.004]. In CCP+, 99/372 (27%) MCPJs had only one MRI abnormality; in 68% of these the abnormality was extra-capsular (57% TSV and 11% IT inflammation). No IT sheath was identified in the cadaveric specimens suggesting the MRI findings represent peri-tendonitis rather than TSV. Dye studies indicated no clear communication between the IT and the adjacent joint (figure 1).
Abstract FRI0047 – Figure 1 Axial MRI showing inflammation of the 3rd palmar interosseous tendon and frozen section showing green dye around the interosseous tendon and blue dye within the MCP joint
Conclusions: IT inflammation represents a peri-tendonitis and is present in anti-CCP +at risk individuals and RA patients where it is associated with MCPJ swelling and tenderness. IT inflammation can occur as the lone MRI abnormality in CCP +at risk individuals suggesting the interossei may be an early extra-capsular target in the development of RA.
References:
Acknowledgements: D Glinatsi, M Ostergaard, P Bird
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.5505