fetching data ... 
Background: The arterial uptake of 18fluorine-2-deoxy-d-glucose (FDG) by positron emission tomography-computed tomography (PET/CT) has been used for the diagnosis of giant cell arteritis (GCA). The role for PET/CT in following disease activity and monitoring treatment effects, however, remains unclear
Objectives: To examine the degree of FDG uptake within the large arteries of GCA patients after 1 year of treatment
Methods: We studied a subgroup of patients enrolled in the GiACTA trial.1 Patients received either tocilizumab (TCZ) given weekly or every other week plus a 26 week prednisone taper, or placebo (PBO) plus either a 26- or 52 week prednisone taper. PET/CTs were done according to site feasibility and not as part of the GiACTA protocol. For this analysis, the 2 TCZ and PBO groups, respectively, were combined. Patients had whole-body PET/CT imaging within 16 weeks of week 52 visit. The ascending aorta, carotid artery and subclavian artery territories were assessed by maximum standardised FDG uptake values (mSUV) measurement. For each territory, we calculated average, most diseased segment (MDS) and most diseased slide mSUVs and target background ratios (TBR). PET/CTs were read centrally by investigators blinded to the clinical and treatment data
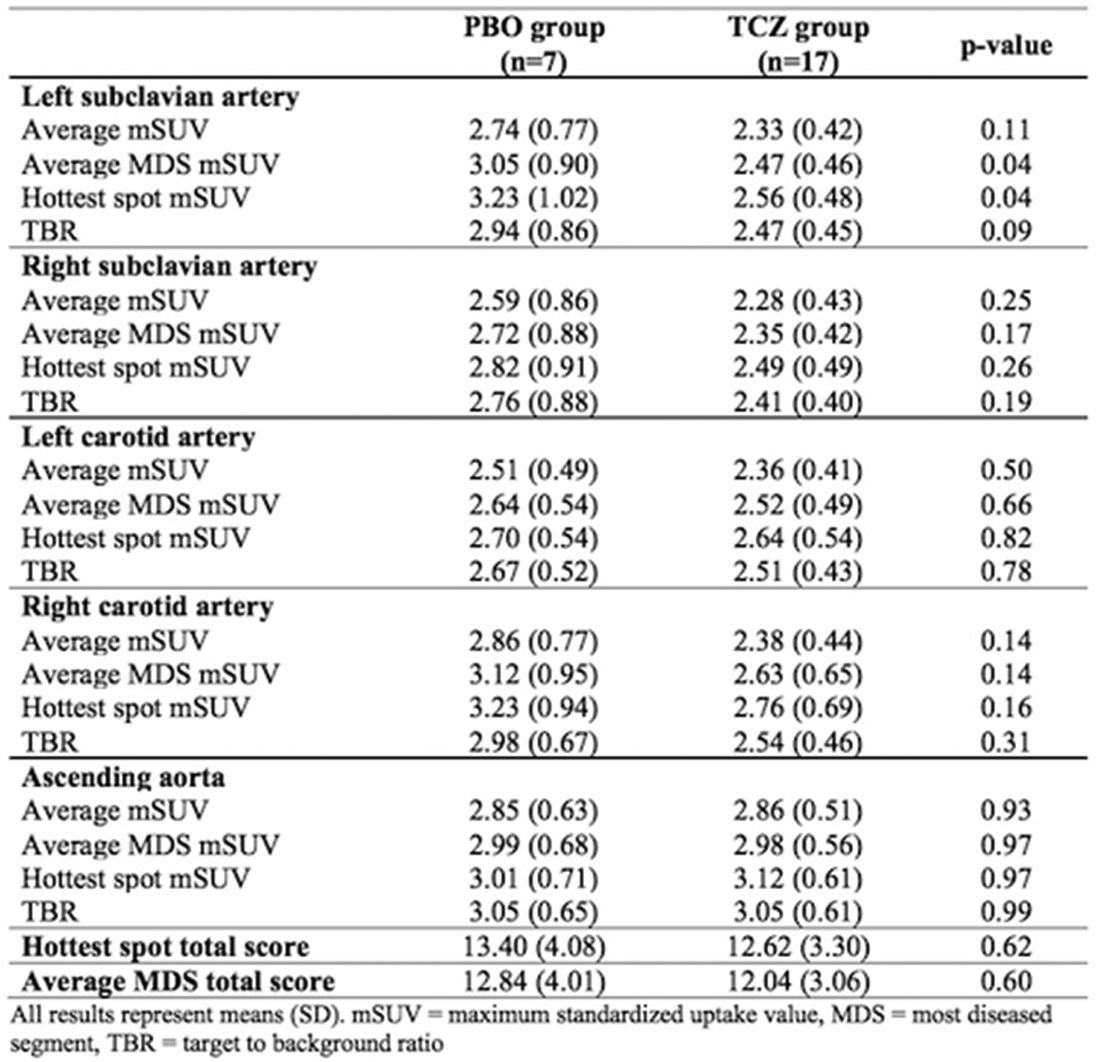
Results: From 251 patients enrolled in GiACTA, 24 patients underwent PET/CT within 16 weeks of week 52 visit. Seventeen patients (71%) received TCZ plus a prednisone taper (TCZ group) and 7 patients received a prednisone taper alone (PBO group). There were no significant differences between groups in baseline characteristics (table 1). Mean (SD) cumulative prednisone dose at week 52 was 2.5 g (1.7 g) in the TCZ group and 3.2 g (1.2 g) in the PBO group (p=0.11). FDG uptake was consistently numerically lower in all vascular territories in TCZ-treated patients compared to PBO-treated patients except in the ascending aorta. However, the between-group differences were statistically significant only in the left subclavian artery (table 2). Adjustment for selected confounders (new onset disease, baseline prednisone dose, prednisone dose at the time of PET/CT, cumulative prednisone dose, flare prior to PET/CT and clinical activity at the time of PET/CT) did not alter the conclusions derived from the univariate analyses
Table 1 Baseline characteristics: All results represent means (SD) except otherwise indicated. PBO=placebo, TCZ=tocilizumab
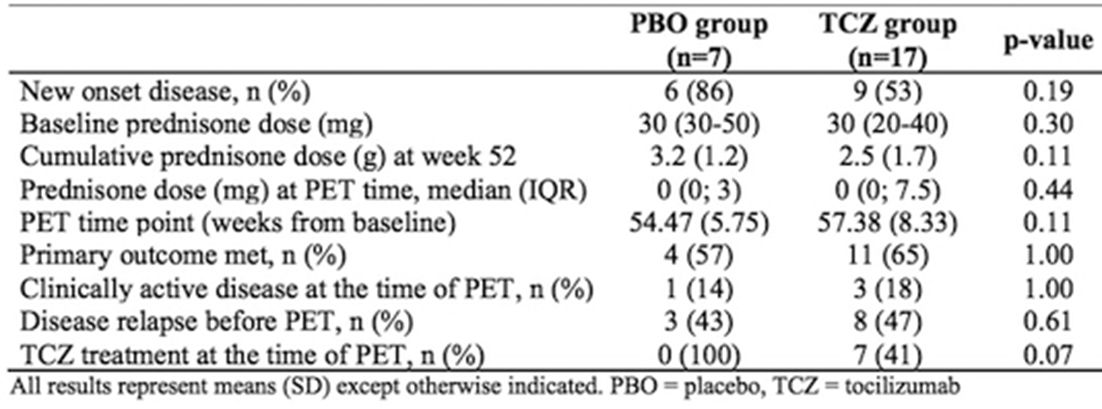
Table 2 Results: All results represent means (SD). mSUV=maximum standardised uptake value, MDS=most diseased segment, TBR=target to background ratio
Conclusions: In this exploratory study, subclavian FGD-uptake was significantly reduced in GCA patients treated with TCZ plus prednisone versus prednisone monotheraphy despite lower cumulative prednisone doses. A larger, carefully designed prospective study is required to fully understand the utility of PET/CT in the longitudinal evaluation of large-vessel vasculitis associated with GCA
Reference:
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.3363