fetching data ... 
Background: Remission is now a realistic and achievable target for many patients with rheumatoid arthritis (RA) using disease-modifying anti-rheumatic drugs (DMARDs) prescribed in modern treat-to-target regimens. However, DMARDs carry risks of potentially serious adverse effects, and require regular and expensive blood monitoring. Recent studies suggest that half of patients with RA in remission can discontinue DMARDs without a flare of arthritis activity, though this cannot currently be reliably predicted.
Demographic |
Value |
|---|---|
Satisfied 2010 ACR/EULAR classification criteria: n (%) |
44 (100%) |
Age: median (IQR) [range] |
66.5 (54.5–71.3) [35 – 82] |
Female: n (%) |
23 (52%) |
Years since RA diagnosis: median (IQR) [range] |
5.5 (3–11) [1–40] |
Seropositive (rheumatoid factor and/or anti-citrullinated peptide antibody): n (%) |
32 (73%) |
Current methotrexate use: n (%) |
38 (86%) |
Baseline DAS28-CRP: median (IQR) [range] |
1.07 (0.99–1.63) [0.96–2.34] |
ACR/EULAR Boolean remission: n (%) |
29 (66%) |
Presence of joint erosion on baseline 7-joint ultrasound scan: n (%) |
29 (70%) |
Objectives: To identify baseline biomarkers that can predict sustained drug-free remission (DFR) versus arthritis flare following DMARD cessation.
Methods: Patients with established RA satisfying clinical (disease activity in 28 joints with CRP [DAS28-CRP]<2.4) and ultrasound (absence of power Doppler synovitis on a blinded 7-joint scan) remission criteria discontinued conventional synthetic DMARDs (methotrexate, sulfasalazine, and/or hydroxychloroquine) and were monitored for 6 months. The primary outcome was time-to-flare, defined as DAS28-CRP≥2.4. Baseline clinical and ultrasound parameters (synovial/tenosynovial greyscale and joint erosions), circulating levels of 26 cytokines/chemokines, and gene expression by peripheral CD4 +T cells (RNA sequencing) were assessed for their ability to predict time-to-flare and flare/DFR status by multivariate Cox regression and receiver-operating characteristic (ROC) analysis.
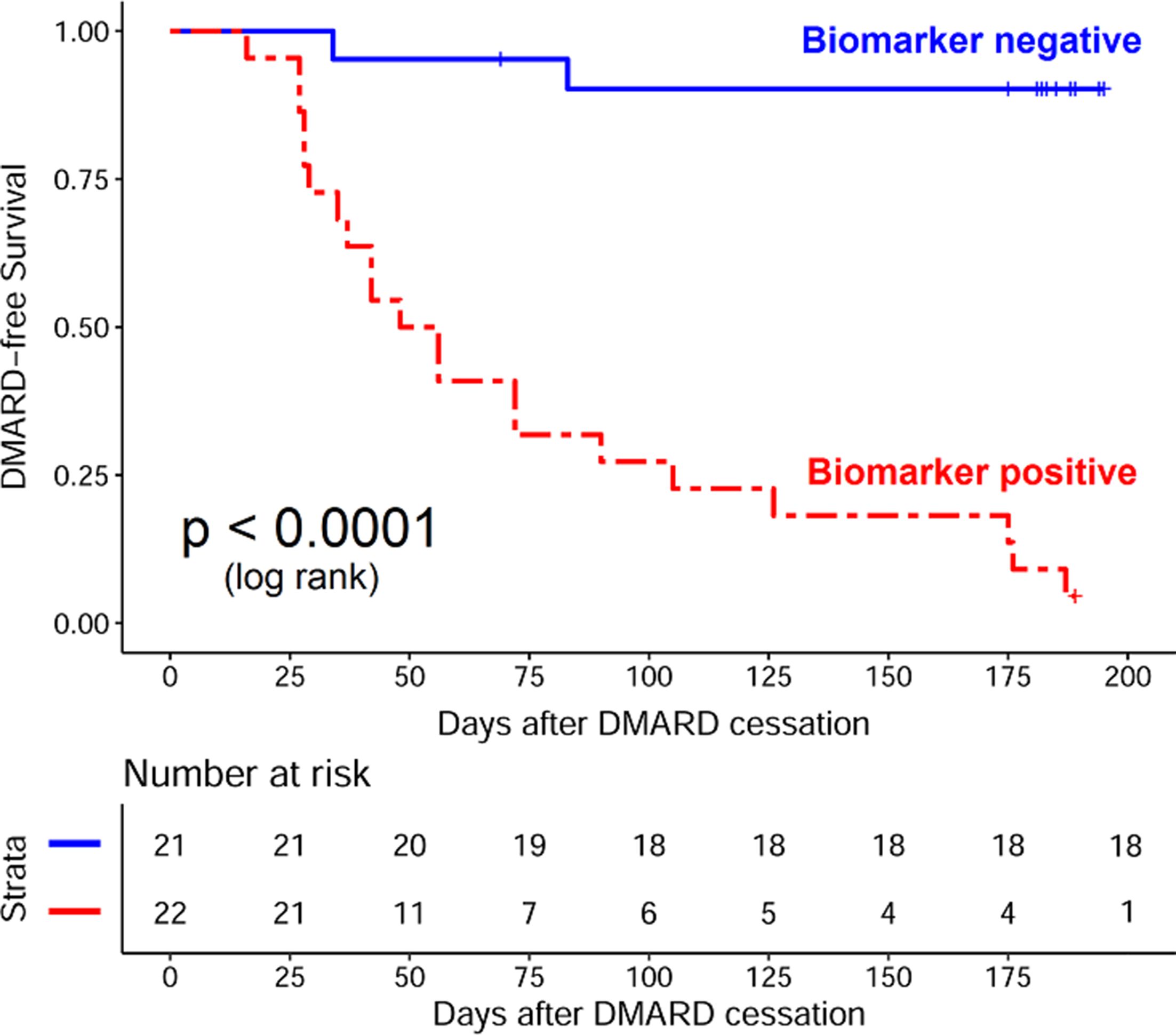
Results: 44 patients were eligible for DMARD cessation (table 1); 23 (52%) experienced an arthritis flare at a median (IQR) of 48 (31.5–86.5) days. A composite score incorporating five variables (three genes [currently subject to patent application], one cytokine [IL-27], and one clinical [ACR/EULAR Boolean remission]) differentiated future flare and DFR with an area under the ROC curve of 0.96 (95% CI: 0.92 to 1.00), sensitivity 0.91 (0.78–1.00) and specificity 0.95 (0.84–1.00) (figure 1).
Conclusions: Our study provides proof-of-concept evidence for the existence of biomarkers of DFR in RA. If validated in an external cohort, these biomarkers may hold promise in guiding DMARD withdrawal, with consequent minimisation of medication adverse events and healthcare costs.
Acknowledgements: KB was supported by the Wellcome Trust [102595/Z/13/A] and the NIHR Newcastle Biomedical Research Centre [BH136167/PD0045]. A patent application is currently in process regarding the gene expression biomarkers, the identify of which will subsequently be disclosed.
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.2775