fetching data ... 
Background: B-cell depletion is a fundamental effect of rituximab (RTX). The speed/depth of initial B-cell depletion is associated with clinical response, and non-responders largely having incomplete depletion.1 2 However, some patients with incomplete depletion still show clinical improvement (ID-R). Little is known about factors associated with complete depletion; the long-term outcome of the two responder groups according to their level of depletion has not been studied yet.
Objectives: To assess factors that are associated with complete depletion and clinical response (CD-R) and compare the 3 year RTX retention between the two RTX responder groups (CD-R vs ID-R), with a view to inform practice on the optimal use of RTX in RA.
Methods: A prospective observational study was conducted in patients with RA who were treated with RTX in Leeds. Each initial cycle of RTX consisted of 2 × 1000 mg infusions, repeated either on clinical relapse or fixed 6 monthly retreatment strategy. B-cells were measured at 0, 2 weeks and every 6 months using highly sensitive flow cytometry (as previously described). Complete depletion was defined as total B cell count <0.0001×109/L at week 2. Patients were classified into 4 groups based on B-cell depletion (CD=complete,) and EULAR response (R=good/moderate, NR=no response). Multiple imputation was used for missing data. Factors for predicting CD-R in cycle 1 (C1) were tested using logistic regression analyses. In the survival analysis, an event was defined as RTX cessation either due to death, safety or switching to other biologics.
Results: A total of 693 patients were treated with RTX in Leeds. Of these, 624 had clinical data at 6 months and were included in the analysis. Total follow-up was 2826 patient-years. In cycle 1, 418/624 (67%) had EULAR response. Of these, 242/418 (58%) had CD-R. In univariable analysis, age, concomitant MTX/LEF, non-smoker, pre-RTX lower naïve, memory B-cell and plasmablasts were associated with CD-R in C1. However, in a multivariable analysis, only concomitant MTX/LEF (OR 2.1 95% CI: 1.3 to 3.5), non-smoker (1.6, 1–2.6) increased the odds while lower plasmablasts (0.89, 0.83–0.95) decreased the odds of CD-R. After adjusting for confounders including age, gender, concomitant MTX/LEF and previous exposure to TNF-i, there was a trend to longer maintenance on RTX (surrogare for response) in the CD-R vs ID-R groups; HR 0.70 (95% CI: 0.46 to 1.05); p=0.058 (figure 1).
Abstract OP0109 – Figure 1 Rituximab retention 3 years after the administration of the first cycle
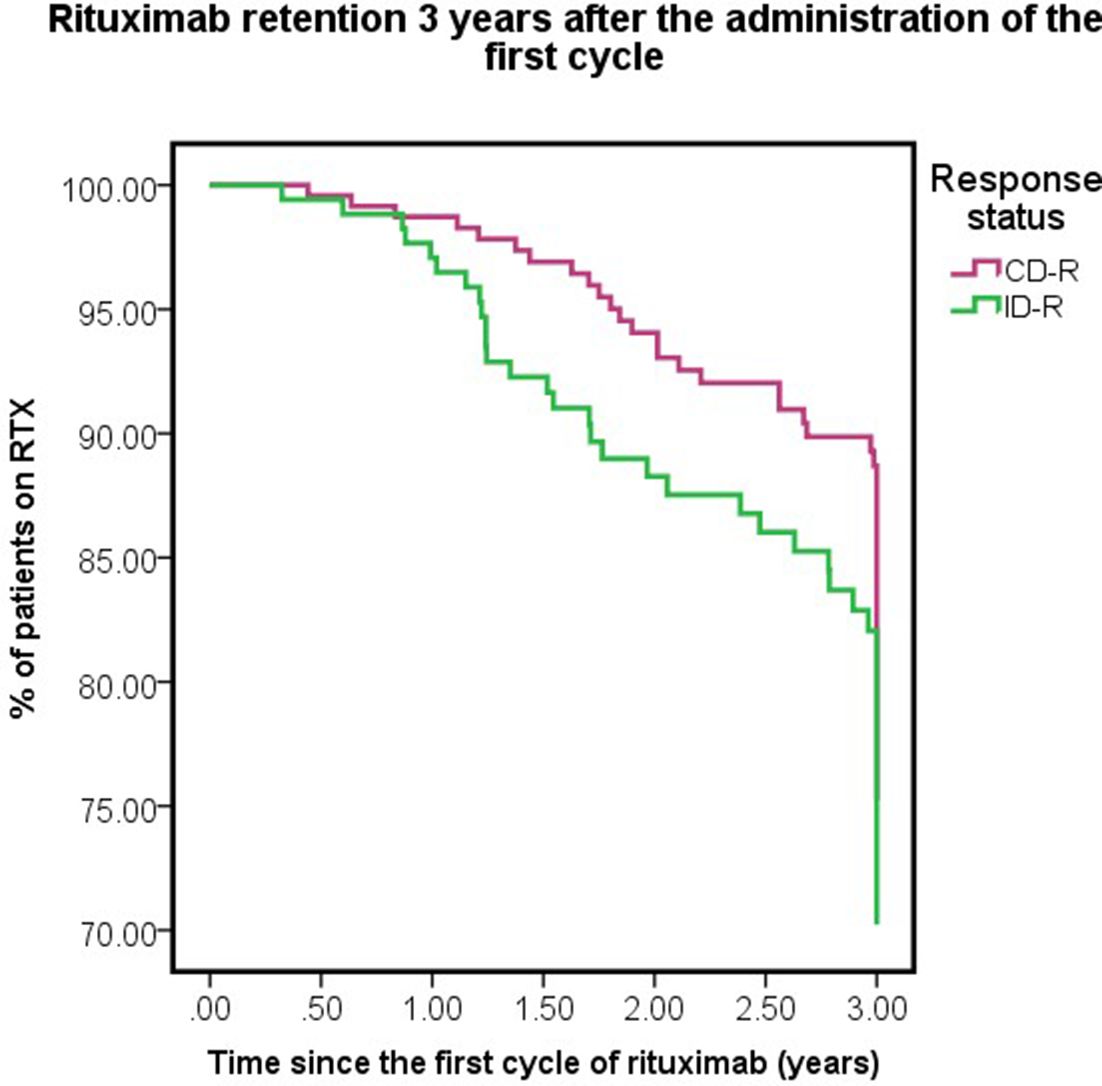
Conclusions: Among patients with good initial clinical response to RTX, we observed differences in immunological response. This had important long term consequences: in patients with early complete B-cell depletion accompanied by good clinical response, RTX treatment was sustained over 3 years numerically, while responses of ID were less durable. Therefore, treatment with anti-CD20 mAb should aim to achieve CD for sustained maintenance on rituximab. CD-R can be predicted by concomitant use of MTX/LEF, non-smokers and those with low baseline plasmablasts.
References
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.5387