fetching data ... 
Background: In addition to glomerular lesions, renal vascular involvement is an important prognostic marker of lupus nephritis (LN). Among patients with various vascular changes, individuals with thromboticmicroangiopathy (TMA) present with severe clinical manifestations and have a high mortality.
Objectives: We sought to assess renalout comes and response to anti-thrombotic treatmentsin addition to conventional immunosuppression in patients with biopsy proven LN and TMA.
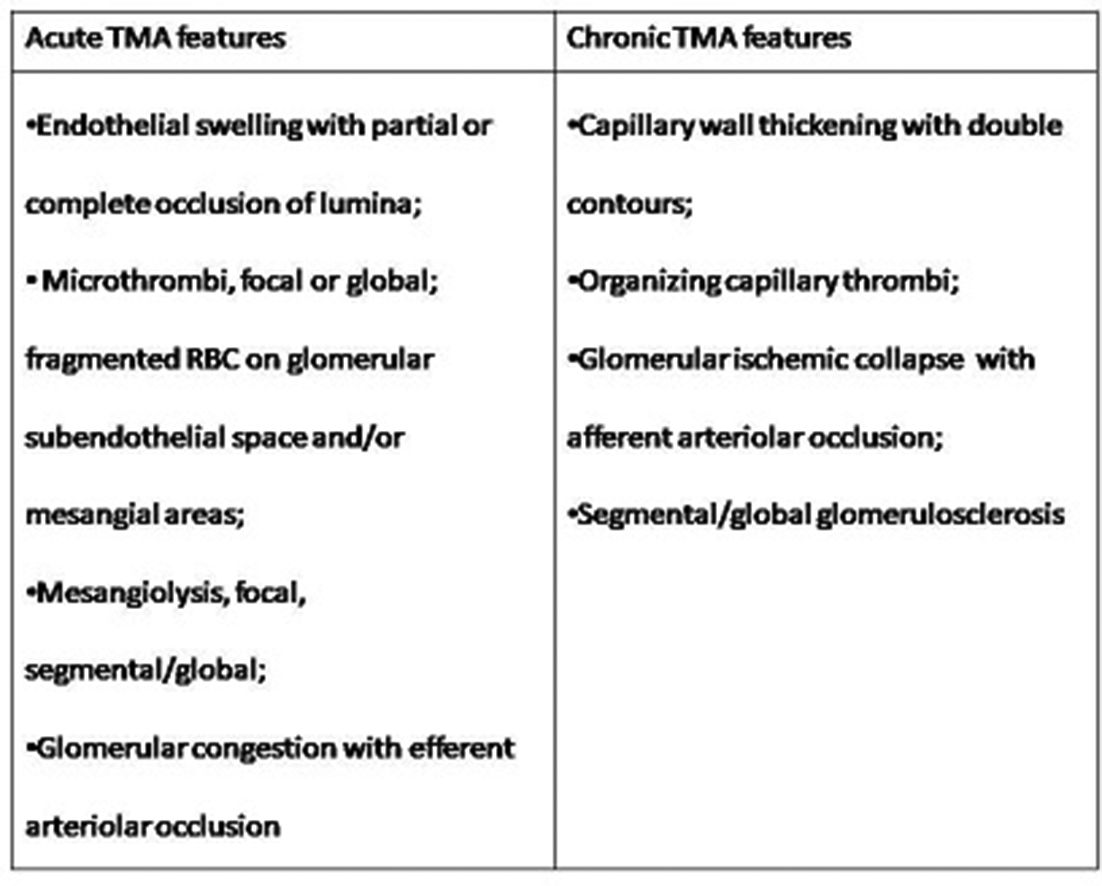
Methods: Clinical and renal histopathological data for 97 patients with biopsy-proven LN and TMA were retrospectively analysed. Antibody profiles, induction and maintenance therapies for LN, and anti-thrombotic treatments were collected. TMA lesions were classified into acute and chronic (table 1). A complete renal response (CR) was defined as proteinuria <0.5 g/24 hour and normal or near-normal (within 10% of normal GFR if previously abnormal) GFR. Partial Response (PR) was defined as a≥50% reduction in proteinuria to subnephrotic levels and normal or near-normal GFR. Renal outcomes were assed at one year post biopsy.
Results: The mean age of the patients was 38.9±15.2 years (range, 13–69 years). The study included 85 females (87.6%) and 12 males (12.4%). The clinical presentations were nephrotic syndrome, nephritic syndrome, and asymptomatic urinary abnormalitiesin 38 (39.2%), 20 (20.6%), 39 (40.2%) patients, respectively. Nine patients were classified Class III (9.3%, including 2 as ClassIII +V), 82 as Class IV (84.5%, 10 as Class IV-segmental(IV-S) (10.3%) and 72 as Class IV-global (IV-G) (74.2%),including 4 as Class IV-G+V) and 6 as Class V (6.2%). Forty-two(43%) patients presented with acute and 55 (57%) with features of chronic TMA. All patients had received treatment with standard immunosuppressants (55% mycophenolate, 39% cyclophosphamide, 6% other regimen) and steroids.
Abstract OP0201 – Table 1
At 12 months, CR was observed in 37 patients (38.1%), PR in 22 (22.6%) and no response in 38 (39.1%). Sixty-one patients (62.9%) were antiphospholipid positive (aPL) and 37 (38.1%) received anticoagulation with vitamin-K antagonist (VKA) and/or heparins. Presence of aPLs(OR, 2.4; 95% confidence interval-CI-, 1.2–7.3; p=0.03), anti-DNA positivity (OR, 12.8; 95% CI: 3.0 to 71.3; p=0.002), and chronic features of TMA (OR, 3.0; 95% CI: 1.2 to 17.5; p=0.04) were all found to be associated with no response. When limiting the analysis to aPL positive patients, after adjusting for type of immunosuppressant therapy and LN class on biopsy, variables that were significantly associated with CR +PR were features of acute TMA rather than chronic (OR, 8.62; 95% CI: 1.4 to 97.1; p=0.03) and the use of VKA/heparins(OR, 2.1; 95% CI, 1.02–16.2; p=0.046)
Conclusions: In patients with concomitant LN and TMA, the presence of aPL and chronic features of TMA were associated with poorer renal outcomes. In patients with aPL, the use of anticoagulation appeared protective and warrants further investigation as a therapeutic tool, especially in the setting of acute TMA.
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.6216