fetching data ... 
Background: Hydrotherapy is recommended in the United Kingdom (UK) by the National Institute for Health and Care Excellence (NICE) as an adjunctive therapy in the management of Axial Spondyloarthritis (AS).1 Despite these guidelines, NHS hospital hydrotherapy services are in decline. The impact on utilisation and patient experience are poorly understood.
Objectives: To identify the utilisation of hospital hydrotherapy services for AS in the UK and capture the patients‘ experience to inform future services and research.
Methods: An online survey was distributed to the National Ankylosing Spondylitis Society (NASS) patient membership between September and November 2017, with social media updates. The survey design included open and closed questions. Thematic analysis of the qualitative responses was conducted.
Results: 250 members completed the survey (40.4% male; average age 50.4 years; average delay to diagnosis 11.4 years). Utilisation: 157 (65.7%) accessed a hospital hydrotherapy service. 102 (63.0%) were referred by rheumatology, 26 (16.0%) via a specialist AS Physiotherapist and 3 (1.9%) self-referring via a telephone helpline. The most frequent service offered was six weekly sessions. 85 (62.5%) reported no access to hospital hydrotherapy when in flare. Barriers to access in a flare included long waiting times, a limit on the sessions offered and pool closures. ‘Pay as you Go’ hospital hydrotherapy sessions were accessed by 35 (16.1%) with 119 (77.3%) interested in doing so. 59 (26.9%) received written hydrotherapy resources for continuation in a non-hospital pool following discharge. 77 (50.7%) were advised to continue with hydrotherapy for self-management. Barriers to utilising a non-hospital pool were high cost, lower pool temperature, pool crowding and a lack of knowledge of exercises. 28 (18.5%) reported a current threat of closure of their hospital hydrotherapy pool. Experience: Five themes emerged from the qualitative data. 1) Emotional well-being: Patients described greater control over their condition when exercising in water. 2) Exercise Behaviour: Patients performed a wider variety of exercise, often challenging themselves, and not attempted on land. 3) Group Effect: Patients described a sense of motivational support when exercising with others. 4) Professional Support: Patients cited the benefit of hydrotherapy sessions led by a physiotherapist who shared their expertise and discussed problems.5) Pool Environment: Patients described gains from non-impact exercise and weightlessness in the water. The warmer pool temperature was stated as a reason for the benefits obtained.
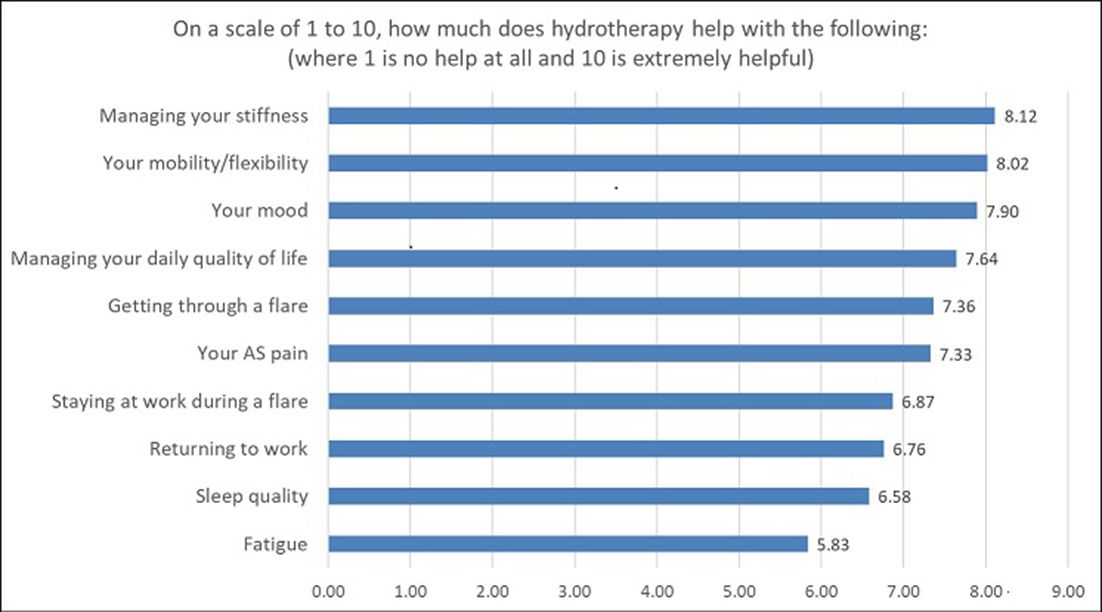
Reported benefits of hydrotherapy are illustrated in graph 1:
Conclusions: This survey suggests variability in utilisation of hospital hydrotherapy services by a national AS patient group in the UK, with barriers to access, lack of promotion and pool closures. Similar benefits of hydrotherapy to those stated in the NICE guidance were experienced.1 Future service recommendations which focus on flexible access for flare management, ‘Pay as you Go’ schemes, group exercise and self-management may increase utilisation, optimise experience and reverse decline. Research to assess the benefits of these service recommendations in a clinical population is needed.
References:
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.3534