fetching data ... 
Background: Rituximab in combination with glucocorticoids (GC) is approved to treat adult patients (pts) with GPA or MPA; however, limited data exist on the safety and efficacy of rituximab in paediatric pts with these potentially life- and organ-threatening diseases.
Objectives: To report the interim safety, pharmacokinetics (PK) and exploratory efficacy data from the 6 month remission induction phase of a Phase IIa international, open-label, 18 month clinical study of rituximab in paediatric pts with GPA or MPA.
Methods: Pts aged ≥2 to≤18 years with newly diagnosed or relapsing GPA/MPA received 4 intravenous (IV) rituximab infusions of 375 mg/m2 body surface area (BSA) on Days 1, 8, 15 and 22 with concomitant GC 1 mg/kg/day (max 60 mg/day) tapered to 0.2 mg/kg/day minimum (max 10 mg/day) by Month 6. All pts received 3 doses of pulse IV methylprednisolone (30 mg/kg/day, max 1 g/day) prior to first rituximab infusion and mandatory prophylaxis for Pneumocystis jiroveci infection. Pts were also pre-medicated with acetaminophen and an antihistamine, 1 hour before each rituximab infusion. Adverse events (AEs) and laboratory data were measured at each study visit (1, 2, 4 and 6 months). Plasma samples for PK analysis were collected throughout the study; clearance and area under the curve (AUC) were calculated using population PK modelling from the RAVE study of rituximab in adult pts with GPA/MPA.1 For exploratory efficacy assessment, the Paediatric Vasculitis Activity Score (PVAS) was measured at each study visit.
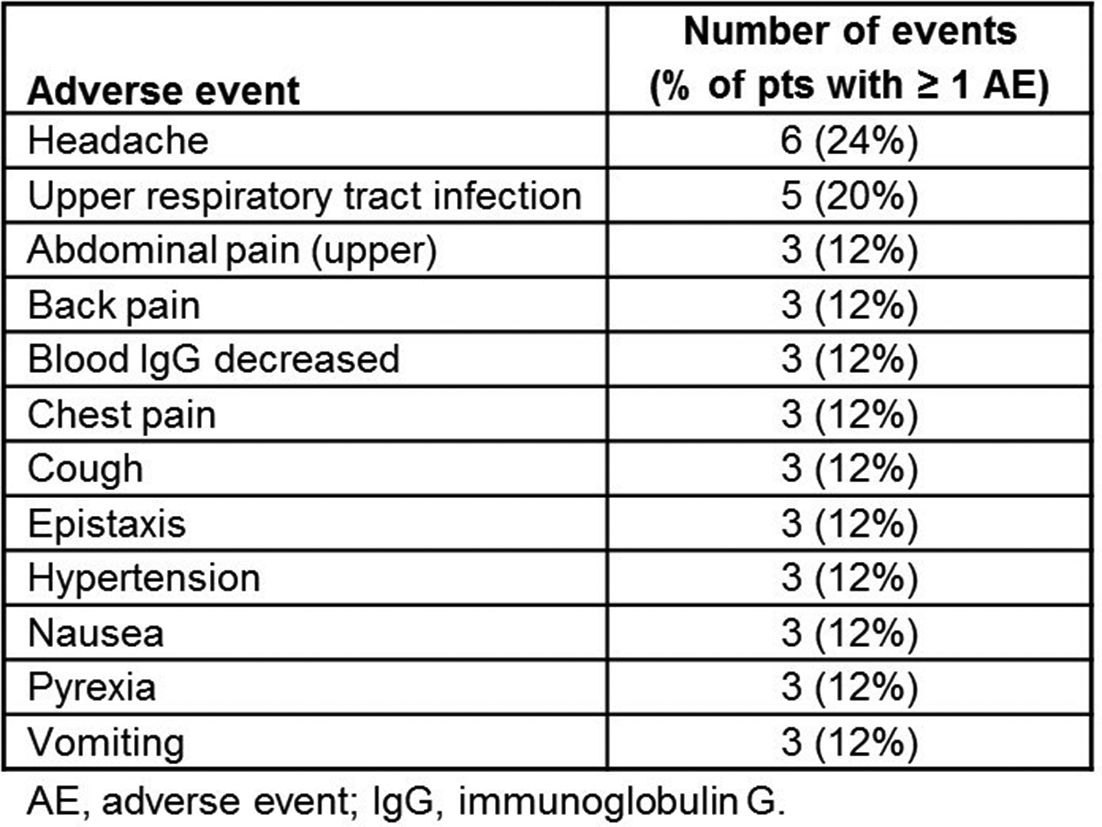
Results: Of the 25 pts enrolled, 19 (76%) had GPA and 6 (25%) had MPA (median [range] age 146–17 years; 80% female). Median (range) disease duration was 0.5 (0.2–0.72) months; 2 pts had received prior cyclophosphamide therapy. All received 4/4 rituximab infusions and completed the 6 month induction phase. By Month 6, all pts had experienced ≥1 AE. The most common AEs by system organ class were infections and infestations in 16 pts (64%). AE terms reported in ≥3 pts are listed in the table 1. Eleven serious AEs occurred in 7 pts (28%), including 3 serious infections (viral gastroenteritis, one lower and one upper respiratory tract infection). 32% of pts had ≥1 infusion related reaction (IRR). No serious IRRs or deaths were reported. The relationship between AUC and BSA was flat and comparable to adult pts. A total of 13 pts (52%) achieved remission by 6 months, defined as PVAS of 0 and GC dose 0.2 mg/kg/day (max 10 mg/day) or PVAS of 0 on 2 consecutive readings≥4 weeks apart irrespective of GC dose.
Abstract OP0332 – Table 1 Adverse events reported in ≥3 patients
Conclusions: In the initial 6 months of this first global clinical trial of rituximab in paediatric pts with GPA/MPA, rituximab was generally safe and well tolerated. The overall safety profile and PK parameters were comparable to adults with GPA/MPA. No new safety signals were observed. However, the study size and interim nature of the analysis limit firm conclusions. The clinical trial and additional efficacy, PK and safety analyses are ongoing.
References:
Acknowledgements: This study is funded by F. Hoffmann-La Roche.
Disclosure of Interest: P. Brogan Grant/research support from: Roche, SOBI, Novartis, Chemocentryx, Consultant for: Roche, SOBI, UCB, Speakers bureau: SOBI, Novartis, G. Cleary Speakers bureau: AbbVie, O. Kasapcopur: None declared, S. Rangaraj: None declared, R. Yeung Consultant for: Novartis, Eli Lilly, P. Brunetta Shareholder of: Roche, Employee of: Genentech, Inc., J. Cooper Employee of: Genentech, Inc., P. Pordeli Employee of: Roche, P. Lehane Employee of: Roche
DOI: 10.1136/annrheumdis-2018-eular.2150