fetching data ... 
Background: Tofacitinib is an oral Janus kinase inhibitor for the treatment of rheumatoid arthritis (RA) and psoriatic arthritis (PsA), which has also been evaluated in other inflammatory rheumatic diseases (IRD) including ankylosing spondylitis (AS). Pain contributes substantial morbidity in patients (pts) with IRD and directly impacts treatment adherence, assessment of disease improvement and health-related quality of life.
Objectives: To evaluate the effectiveness of tofacitinib in reducing pain in randomised controlled clinical trials in pts with RA, PsA and AS.
Methods: Five pt populations treated with tofacitinib 5 mg twice daily (BID), 10 mg BID or placebo (PBO) were evaluated: [1] conventional synthetic disease-modifying antirheumatic drug (csDMARD)-inadequate response (IR) RA pts pooled from ORAL Scan (NCT00847613), ORAL Sync (NCT00856544) and ORAL Standard (NCT00853385), [2] tumour necrosis factor inhibitor (TNFi)-IR RA pts from ORAL Step (NCT00960440), [3] csDMARD-IR PsA pts from OPAL Broaden (NCT01877668), [4] TNFi-IR PsA pts from OPAL Beyond (NCT01882439) and [5] AS pts from a Phase 2 study (NCT01786668). Pain outcomes evaluated from baseline to Month (M)6 (Week [W]12 in the AS population) included Pt’s Assessment of Arthritis Pain (PAAP) (RA and PsA populations only), Short-Form Health Survey (SF)-36v2 Q7 (bodily pain in the past week), SF-36v2 Bodily Pain Domain (BP), EuroQol Five Dimensions Questionnaire Pain/Discomfort Domain (EQ-5D PD; all populations) and Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) Q2 (level of AS neck, back or hip pain) and Q3 (other pain) score (PsA and AS populations only; PsA pts had presence of spondylitis at screening and baseline BASDAI total score >0 in the full analysis set [FAS]). Data were analysed descriptively.
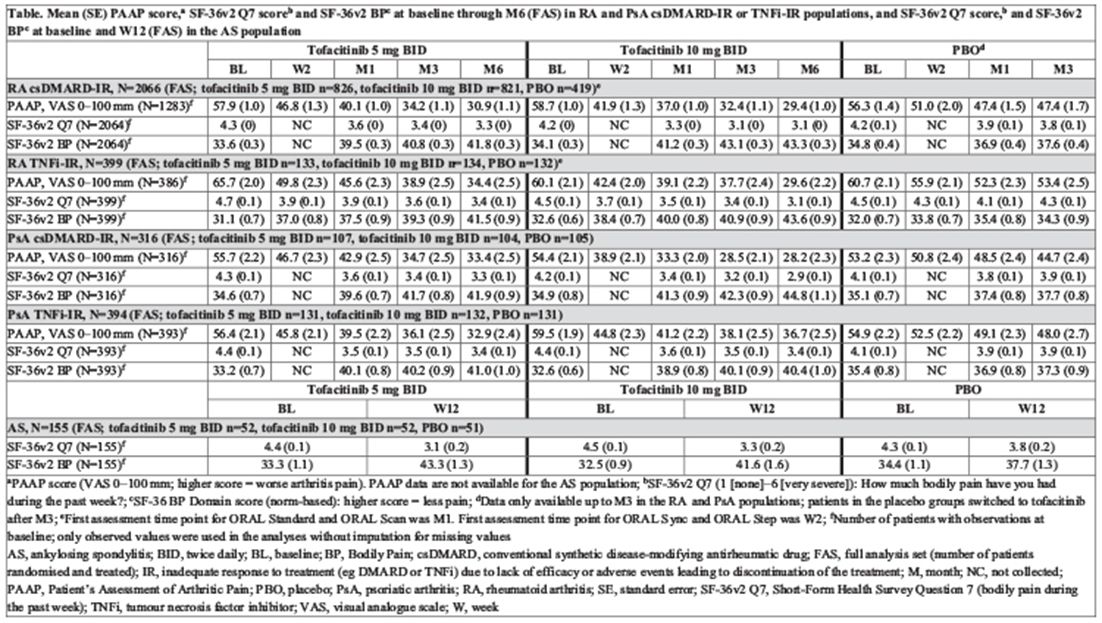
Results: The csDMARD-IR RA, TNFi-IR RA, csDMARD-IR PsA, TNFi-IR PsA and AS populations comprised a total of 2066, 399, 316, 394 and 155 pts in the FAS, respectively. In each RA or PsA csDMARD-IR and TNFi-IR population treated with tofacitinib, mean PAAP at baseline (5 mg BID, range 55.7–65.7 mm; 10 mg BID, 54.4–60.1 mm) decreased as early as W2 (1st post-baseline assessment; 45.8–49.8 mm; 38.9–44.8 mm) and continued to decrease through M6 (30.9–34.4 mm; 28.2–36.7 mm); decreases were numerically greater vs PBO and the magnitude of change in RA and PsA populations was similar (Table). Improvements in SF-36v2 Q7 (Table), SF-36v2 BP (Table) and EQ-5D PD were observed in all 4 RA and PsA csDMARD-IR and TNFi-IR populations, and in BASDAI Q2 and Q3 in the csDMARD-IR PsA and TNFi-IR PsA populations. In the AS population, improvements from baseline in mean SF-36v2 Q7 (Table), SF-36v2 BP (Table), EQ-5D PD and BASDAI Q2 were reported at W12 and were numerically greater vs PBO.
Table 1 Mean (SE) PAAP score,a SF-36v2Q7 scoreb and SF-36v2 BPc at baseline through M6(FAS) in RA and PsA csDMARD-IR or TNFi-IR population, and SF-36v2Q7 score,b and SF-36v2 BPc at baseline and W12 (FAS) in the AS population
Conclusions: Treatment with tofacitinib is associated with a rapid improvement and sustained reduction of pain in pts with RA and PsA who are csDMARD-IR or TNFi-IR, and in pts with AS.
Acknowledgements: Study sponsored by Pfizer Inc. Medical writing support was provided by P Scutt of CMC and funded by Pfizer Inc.
Disclosure of Interest: A. Ogdie Grant/research support from: Novartis, Consultant for: Novartis, Pfizer Inc, Takeda, K. de Vlam Consultant for: Eli Lilly, Pfizer Inc, I. McInnes Grant/research support from: Celgene, Janssen, Novartis, Pfizer Inc, Roche, UCB, Consultant for: AbbVie, Celgene, Janssen, Novartis, Pfizer Inc, Roche, UCB, P. Mease Grant/research support from: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Lilly, Novartis, Pfizer Inc, Sun, UCB, Consultant for: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Lilly, Novartis, Pfizer Inc, Sun, UCB, Speakers bureau: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Genentech, Janssen, Novartis, Pfizer Inc, UCB, P. Baer Consultant for: AbbVie, Amgen, Janssen, Johnson and Johnson, Lilly, Novartis, Paladin, Pfizer Inc, Sanofi-Genzyme, Takeda, Speakers bureau: Amgen, Janssen, Lifelass, Pfizer Inc, T. Lukic Shareholder of: Pfizer Inc, Employee of: Pfizer Inc, K. Kwok Shareholder of: Pfizer Inc, Employee of: Pfizer Inc, C. Wang Shareholder of: Pfizer Inc, Employee of: Pfizer Inc, M.-A. Hsu Shareholder of: Pfizer Inc, Employee of: Pfizer Inc, A. Maniccia Shareholder of: Pfizer Inc, Employee of: Pfizer Inc
DOI: 10.1136/annrheumdis-2018-eular.3247