fetching data ... 
Background: Pain is a common and debilitating feature of rheumatoid arthritis (RA) and a level >40 mm on a Visual Analogue Scale (VAS) of pain (scale 0–100 mm) has been suggested as a measure of unacceptable pain.1 While many studies have focused on the effect on inflammation of different pharmacological options, few earlier reports have directly compared pain outcomes between common treatment strategies.
Objectives: The aim of this study was to investigate pain development and unacceptable pain over 2 years after start of biological as compared to conventional combination therapy in early RA patients.
Methods: The multicentre SWEFOT (SWedish FarmacOTherapy) trial was designed as a randomised, active-controlled, open-label study, enrolling new-onset (<1 year) patients fulfilling 1987 American College of Rheumatology criteria for RA Oct 2002 to Dec 2005. After a 3 month run-in period on methotrexate (MTX), patients who did not reach low disease activity (Disease Activity Score using 28-joint count; DAS28 ≤3.2) were randomised to addition of infliximab (IFX) or sulfasalazine +hydroxychloroquine (SSZ +HCQ). Results for disease activity, radiographic data and health-related quality-of-life have been published earlier.2,3 Here, unacceptable pain (VAS pain >40 mm) at 2 years follow-up and area under the curve (AUC) for VAS pain were used as outcome measures. We used intention-to-treat with last observation carried forward in case of protocol breach as study approach. Statistical analyses were performed by logistic regression for unacceptable pain and analysis of covariance for AUC for VAS pain, adjusting for age, sex, and VAS pain at randomisation.
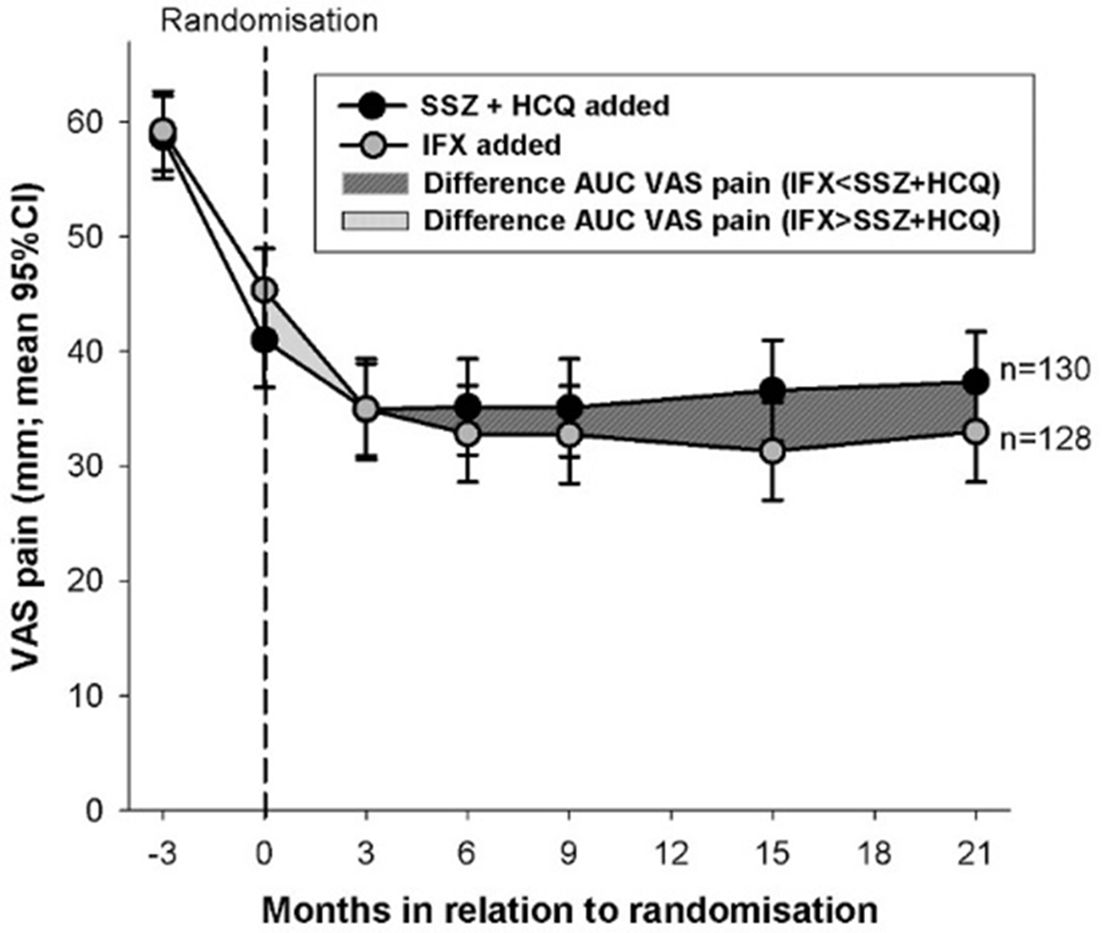
Results: 487 RA patients were enrolled of whom 258 (who did not respond sufficiently to MTX) were randomly allocated to either addition of IFX (n=128) or SSZ+HCQ (n=130). Baseline characteristics were similar between the two groups. Out of patients assigned to IFX, 32% had unacceptable pain at 2 years follow-up (21 months after randomisation), while the same figure for SSZ+HCQ (n=130) was 45% (adjusted odds ratio 0.41 [95%CI 0.23–0.73]; p=0.003). Serial VAS pain measurements are displayed in figure 1. An AUC analysis for mean VAS pain levels from randomisation to 2 years follow-up confirmed significantly lower levels for patients randomised to IFX compared to SSZ+HCQ (p=0.01).
Conclusions: Despite early active treatment, a large share of new-onset RA patients showed unacceptable pain after 2 years. Interestingly, both the fraction of patients with unacceptable pain and assessment of pain over time were substantially lower for patients randomised to addition of IFX compared to SSZ+HCQ, contrasting to earlier SWEFOT reports where significant between-group differences at 2 years follow-up for disease activity and health-related quality-of-life were not seen.2,3 This suggests a better effect on long term pain for the biological therapy, which could be taken into account when choosing treatment strategy in patients responding insufficiently to MTX.
References:
Disclosure of Interest: T. Olofsson: None declared, J. Wallman Consultant for: AbbVie, Celgene, Eli Lilly, Novartis, UCB, A. Jöud: None declared, M. Schelin: None declared, S. Ernestam: None declared, R. van Vollenhoven Grant/research support from: AbbVie, BMS, GSK, Pfizer, UCB, Consultant for: AbbVie, AstraZeneca, Biotest, BMS, Celgene, GSK, Janssen, Lilly, Novartis, Pfizer, UCB, S. Saevarsdottir: None declared, J. Lampa Grant/research support from: AbbVie, Speakers bureau: AbbVie, Eli Lilly, Hospira, MSD, Novartis, Pfizer, Roche, Sandoz, UCB
DOI: 10.1136/annrheumdis-2018-eular.1844