fetching data ... 
Background: Giant cell arteritis (GCA) is a systemic vasculitis that affecting large and medium vessels, mainly the temporal artery and other arteries of extracranial localization (1).
Objectives: A series of 24 patients with clinical suspicion of GCA proved by a positive temporal artery biopsy (TAB) has been reviewed. Our aim was to asses a) histologic inflammatory patterns in the TAB and b) their possible correlation with analytical and clinical data.
Methods: Prospective study of 24 patients with positive TAB between January of 2016 until January of 2018. Clinical data, included: age, sex, symtomatology (craneal, visual or systemic manifestations) and physical examination of the temporal artery.
The analytical data registered were: ESR, CRP and haemoglobin. Furthermore, it has been considered if patients were receiving treatment with corticosteroids at the time of the biopsy.
Positive biopsies were classified into four categories: a) inflammation limited exclusively to the small vessels of the adventitia (SVV); b) vasa vasorum vasculitis (VVV); c) inflammation limited to the adventitia (ILA); and d) transmural inflammation (TMI). The presence of giant cells, thrombosis and distrophic calcification was also noted.
Results: We included a total of 24 patients with positive TAB: a) 19 patients (79.16%) presented TMI and b) 5 patients (20.84%) presented ILA. There were no cases with SVV or VVV.
No significant differences at baseline were observed between the 2 groups regarding sex and age, with a mean of 79.6 ± 7.2 years in TMI group and 78.8 ± 7.3 years in ILA group (p = 0.83).
There were no significant differences between the correlation of the clinical and analytical data and the 2 patterns of inflammation observed in the biopsy
(
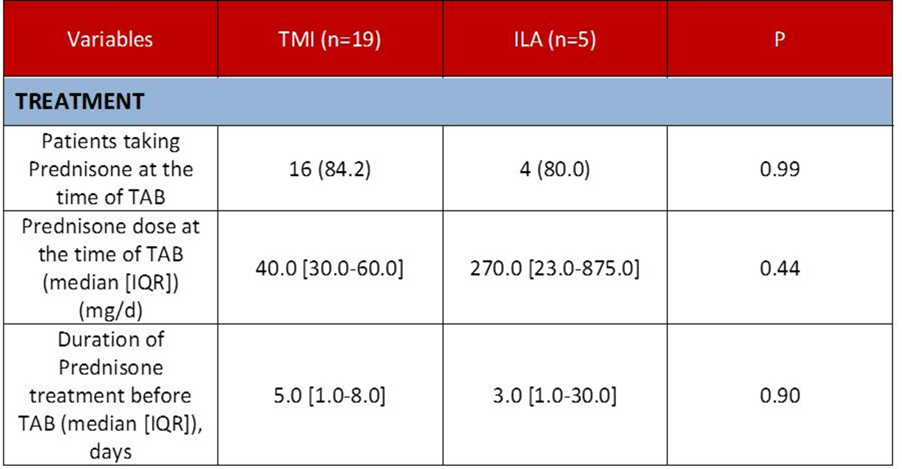
Regarding the treatment at the time of performing the BAT, 16 (of 19) patients in the group with TMI (84.2%) and 4 (of 5) patients in the group with ILA (80%) were receiving treatment with oral glucocorticoid (Prednisone). No significant differences between the two groups were found in terms of treatment duration prior to BAT and nor in the dose recived
(
Conclusion: In our sample, we didn’t observe differences between the patterns of inflammation and the analytical and clinical data. It is important to recognise these patterns of inflammation in the TAB to avoid false negatives.
REFERENCES:
1- MA González-Gay, T Pina, D Prieto-Peña, M Calderon-Goercke, R Blanco, S Castañeda (2018) Current and emerging diagnosis tools and therapeutics for giant cell arteritis,Expert Review of Clinical Immunology, 14:7, 593-605, DOI: 10.1080/1744666X.2018.1485491.
TABLE-1. CLINICAL aND aNALYTICAL DATA.
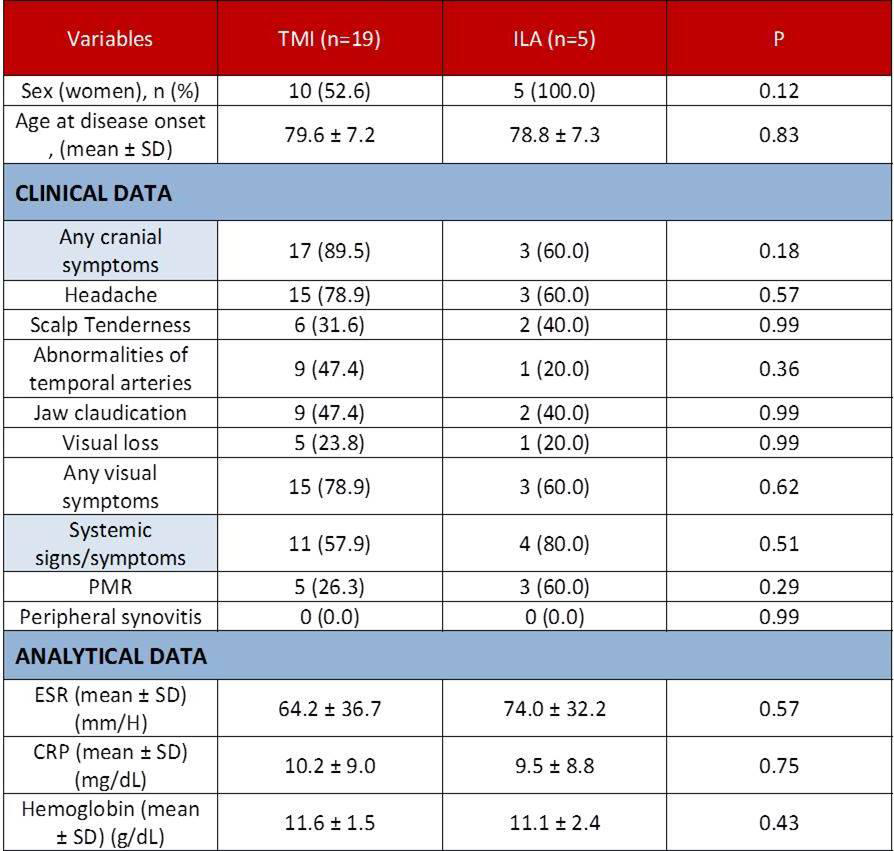
TABLE-2. TREATMENT.
Disclosure of interests: Lara Sánchez Bilbao: None declared, Iñigo González-Mazón: None declared, D. Prieto-Peña: None declared, Monica Calderón-Goercke: None declared, José Luis Martín-Varillas: None declared, Belén atienza-Mateo: None declared, C. González-Vela: None declared, Miguel Á. González-Gay: None declared, Ricardo Blanco Grant/research support from: abbvie, MSD, and Roche, Consultant for: abbvie, Pfizer, Roche, Bristol-Myers, Janssen, Speakers bureau: abbvie, Pfizer, Roche, Bristol-Myers, Janssen
DOI: 10.1136/annrheumdis-2019-eular.6228