fetching data ... 
Background: The usefulness of very low hydroxychloroquine (HCQ) blood levels to unmask severe non-adherence in patients with systemic lupus erythematosus (SLE) has been established, including in a recent prospective study. However, little is known on the individual impact of HCQ blood levels measurement.
Objectives: To assess the impact of HCQ blood levels measurements to detect patients with severe non-adherence and to assess its main causes.
Methods: Retrospective interviews about adherence to treatment were conducted by the same investigator in unselected consecutive SLE patients. Patients were classified as severely non-adherent (groups A and B) or not (group C). Group A included patients in whom the diagnosis of severe non-adherence was first made because of a blood HCQ level less than 200ng/ml at least once during follow-up, and group B because of the patient’s acknowledgment of their complete interruption of HCQ treatment for at least one month. Mean HCQ blood levels were compared during the follow-up. The Medication Adherence Self-report Inventory scale (MASRI) was completed by each patient at the time of the interview (reflecting adherence in the last 30 days).
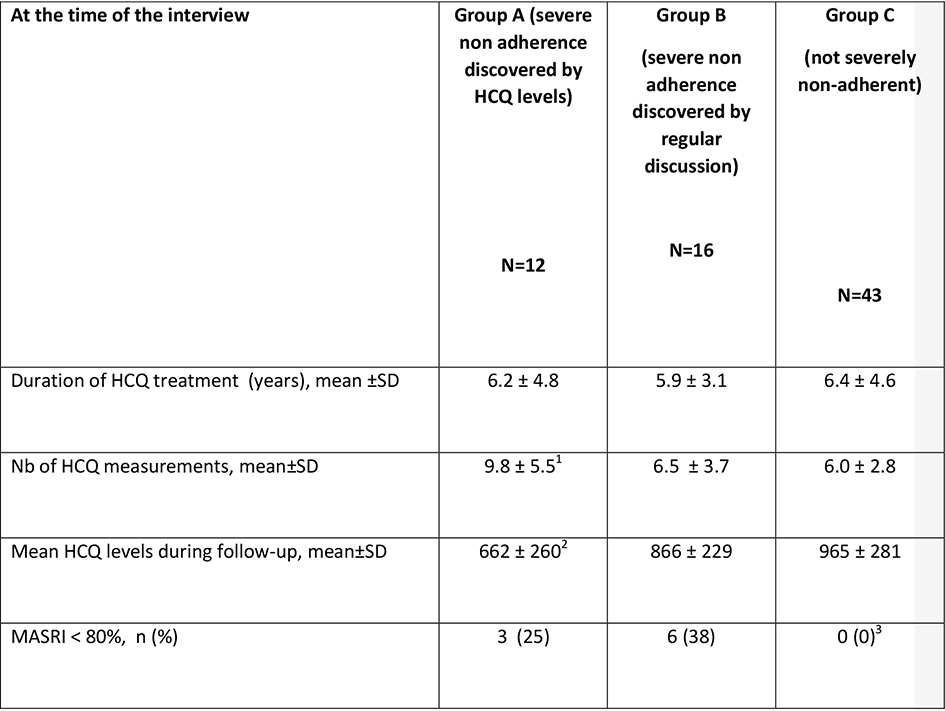
Results: 71 SLE patients who had a mean of 6.8 (±3.8) measurements of HCQ blood levels during a mean follow-up of 6.2 years (± 4.3) were included (Table). Twenty-eight patients (39%) had been diagnosed at some point with severe non-adherence: 12 in group A and 16 in group B (6 (38%) of them also had - at least - one HCQ blood level <200 ng/ml following the recognition of non-adherence). Demographic characteristics were similar between groups ( p =NS, data not show). After the diagnosis of severe non-adherence, the mean±SD HCQ levels (including all the determinations of HCQ levels done before versus those done after this diagnosis) improved in Group A (from 232±249 ng/ml to 761±338 ng/ml; p <0.005) while they remained stable in Group B ( p = NS). Non-acceptance of the disease was the leading cause of severe non-adherence to treatment in Group A (7 patients (58%) versus 2 patients in Group B (12.5%); p =0.02) while the boredom with chronic treatments was the main reported cause in Group B (9 patients (56%) versus 1 patient in Group A (8%); p =0.02).
Conclusion: We provide novel evidence that, in a real-life setting, HCQ blood level measurements are useful to diagnose severe non-adherence since 12 of 28 severly non-adherent patients were diagnosed because of HCQ levels. We confirm that discovering very low HCQ blood levels leads to increase HCQ blood concentrations in the next samples after having stressed (and discussed!) the problem to the patient.
REFERENCES:
HCQ: hydroxychloroquine; 1-2 : p <0.005 versus Group C; 3 : p<0.0005 versus A and B Groups; other p values were non-significant; p values were calculated by unpaired t-tests and Fisher’s exact tests, as appropriate.
Disclosure of Interests: None declared
DOI: 10.1136/annrheumdis-2019-eular.6927