fetching data ... 
Background: The immunology laboratory at Barts Health supports a large clinical myopathy service, providing blood tests for myositis-specific autoantibodies (MSA) by a commercial line immunoblot panel for Jo1, PL7, PL12, SRP, Mi2, Ku, PM-Scl and Scl-70.
As Idiopathic Inflammatory Myositis (IIM) disease subtype definitions have evolved from the 1975 Bohan & Peter criteria, the discovery of new antibodies has proven useful in the hands of neuromuscular clinicians whose patients have a high pre-test probability of disease. Ready availability of the test has led to increased demand from:
Respiratory physicians with patients with severe Interstitial Lung Disease (ILD) which can be a symptom of some IIMs.
The connective tissue disease (CTD) screening section of the laboratory in which many patients are screened for antinuclear antibodies (ANA), which occasionally produces a pattern that may be associated with an MSA.
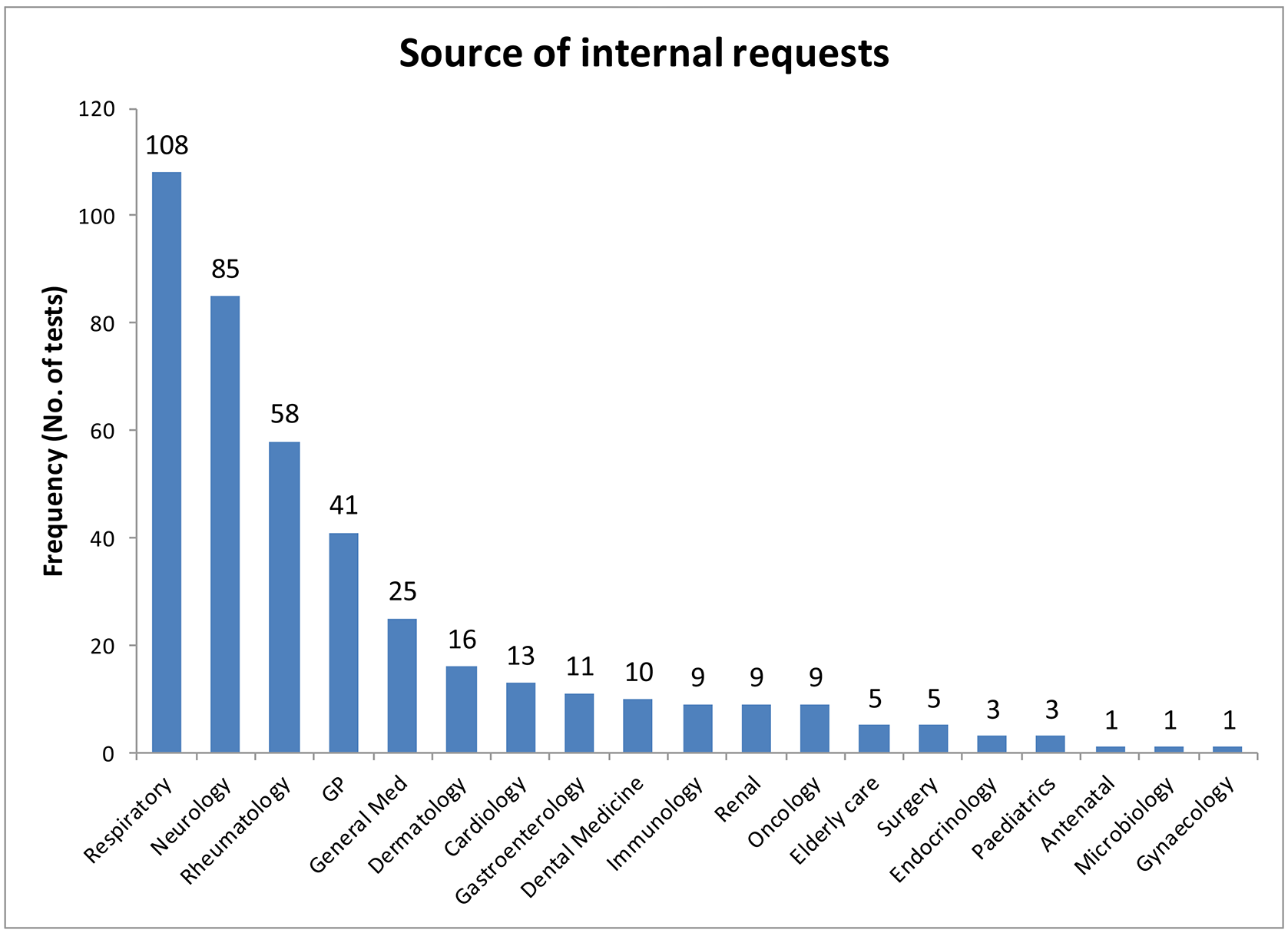
Determine the frequency of MSA requests from different departments.
To investigate the possibility of rejecting requests for MSAs at the laboratory in the absence of an elevated creatine kinase (CK), a hallmark of muscle damage associated with myositis (1).
Methods: MSA were measured by a commercial line blot (Bluediver) which included Jo-1, PL-7, PL-12, Mi-2, Ku, SRP-54 and PM-Scl-100. Demographics and results for all MSA requested between September 2017 and November 2019 were pulled from laboratory records, together with CK results (if performed). CK was interpreted as low, normal or elevated according to reference ranges of 25-200 U/L (female) or 40-320 U/L (male).
Results: 597 tests were performed between 2017 and 2019. In total 59/597 (10%) were positive for the audited antibodies (
| Positive on polymyositis screen | % positivity | |
|---|---|---|
| All tests | 597 | |
| Total | 59 | 9.9% |
| Jo-1 | 4 | 0.7% |
| PL-7 | 2 | 0.3% |
| PL-12 | 5 | 0.8% |
| SRP-54 | 10 | 1.7% |
| Mi-2 | 4 | 0.7% |
| Ku | 3 | 0.5% |
| PM-Scl 100 | 25 | 4.2% |
| Scl-70 | 7 | 1.2% |
MSAs had an associated CK result in 75% of internal and 12% of GP requests. A cohort of 17 patients had positive MSAs (3 x SRP, 1 x PL-7, 1 x Jo-1, 2 x Mi-2, 1 x Ku, 8 x PM-Scl100 and 1 x Scl-70) with normal CK.
Of the 41 GP requests, MSA had been requested by the lab on the basis of ANA pattern for 33 (80%) of them, 3 of which were positive (2 x Scl-70, 1 x SRP-54).
Conclusion: Demand for MSA from the Respiratory department (screening for ILD) currently exceeds demand from Neurology and from Rheumatology. In the GP cohort, 33 requests (80% of GPs, 5% of all requests) were generated by the laboratory.
A cohort of patients with normal CK results had a positive MSA, implying CK alone cannot be used to limit test access. Interestingly, 10 positive results had no CK requested implying they were not being investigated for myositis.
Further work is needed to determine the specificity and sensitivity of these antibodies for patients with clinically defined myositis, and the appropriateness of allowing the test to be applied in the absence of any clinical evidence of IIM.
The findings of this audit need to be further extended to look at other myositis including other anti-synthetases, HMGCoAR, MDA5, TIF-1γ, NPX-2.
REFERENCES:
[1]Dalakas MC, Hohlfeld R (2003) Polymyositis and dermatomyositis. Lancet 362:971–982
Disclosure of Interests: None declared