fetching data ... 
Background: Secukinumab (SEC), an interleukin-17A inhibitor, has demonstrated improvements on multiple domains of psoriatic arthritis (PsA). 1 Adalimumab (ADA), a TNF inhibitor, is widely used as a first–line biologic in PsA.
Objectives: To report efficacy and safety outcomes from the head-to-head EXCEED trial (NCT02745080) that compares SEC vs. ADA as first–line biologic monotherapy through 52-weeks (wks), with a musculoskeletal primary endpoint in pts with active PsA.
Methods: Head-to-head, phase-3b, randomised, double-blind trial: biologic naïve active PsA pts were randomised to receive SEC 300mg subcutaneous at baseline, Wk1-4, and then every 4wks (q4w) until Wk48 or ADA 40mg subcutaneous at baseline and then q2w until Wk50. The primary endpoint was superiority of SEC vs. ADA on ACR20 response at Wk52. Binary and continuous variables were analysed using logistic-regression model and MMRM, respectively. Safety analysis included patients who received ≥1 dose of study-drug.
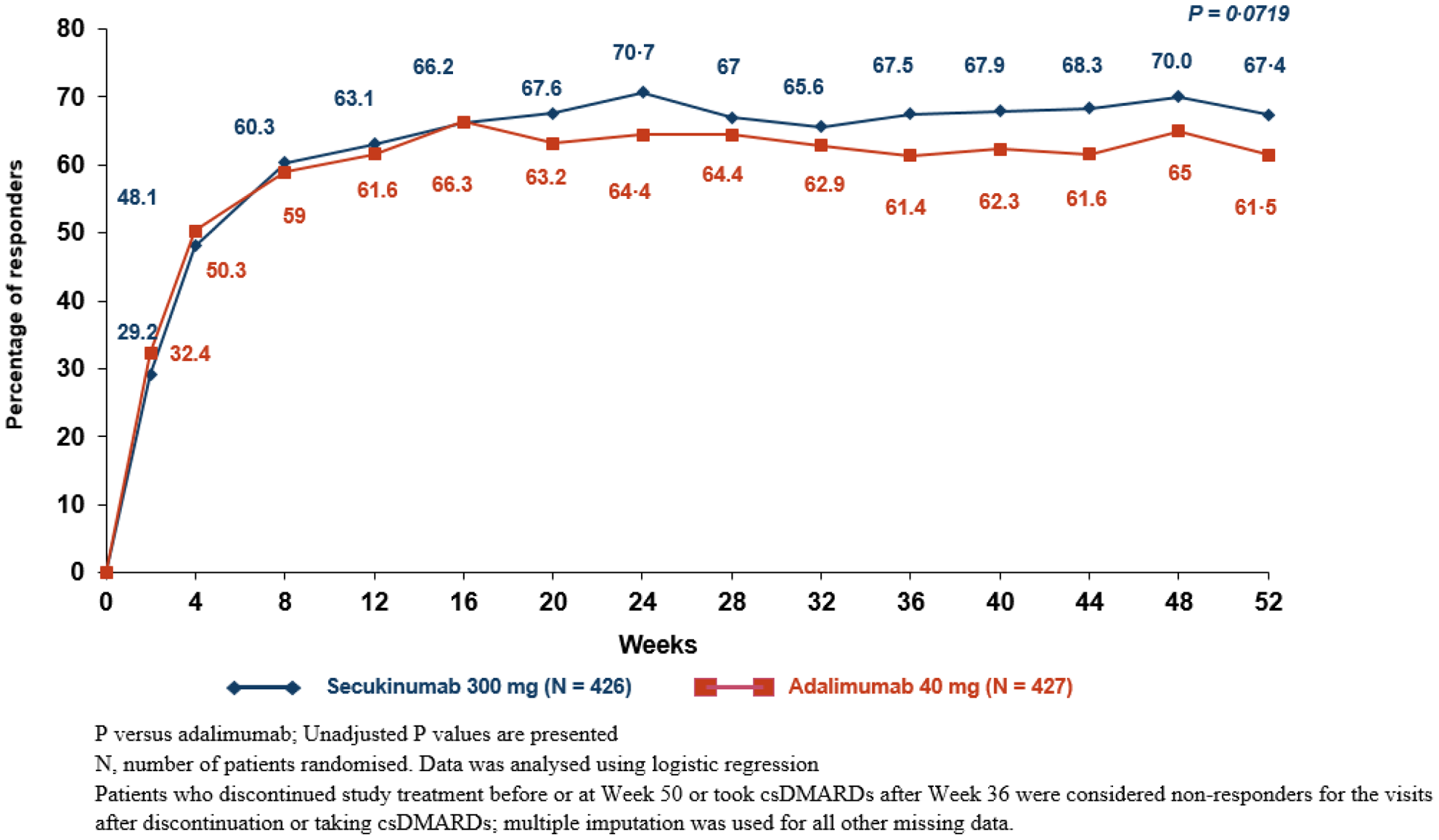
Results: 853 pts were randomised to receive SEC (n=426) or ADA (n=427). Baseline demographics and disease characteristics were comparable between treatment-groups except higher proportion of female pts and pts without enthesitis in the SEC group. ACR20 response at Wk52 for SEC vs. ADA were 67·4% vs. 61·5%, respectively (p=0·0719) (Figure). Higher clinical responses were observed with SEC vs. ADA for a range of musculoskeletal, skin, and higher-hurdle outcomes (Table). A higher retention rate was observed for SEC (85.7%) vs. ADA (76.3%). Safety profiles of SEC and ADA were consistent with previous reports. 2,3
Conclusion: Results suggest that SEC is at least as efficacious as ADA on musculoskeletal endpoints whilst providing higher responses on skin endpoints, and is associated with a higher retention rate. No new safety signals were reported.
REFERENCES:
[1]van der Heijde, et al. Rheumatol. (Oxford).2019; DOI10.1093/rheumatology/kez420.
[2]Deodhar A, et al. Arthritis Res Ther. 2019;21:111.
[3]Burmester GR, et al. Ann Rheum Dis.2013; 72:517-24.
ACR20 Response through Wk 52
Efficacy Outcomes at Wk 52
| Endpoints, % response unless specified otherwise | SEC 300 mg
| ADA 40 mg
| P-value (unadjusted)* |
|---|---|---|---|
| ACR20 | 67·4 | 61·5 | 0·0719 |
| a ACR20 | 66·9 | 59·5 | 0·0239 |
| Key Secondary | |||
| b PASI 90 | 65·4 | 43·2 | <0·0001 |
| ACR50 | 49·0 | 44·8 | 0·2251 |
| HAQ-DI mean change from baseline ± SE | -0·58 ± 0.03 | -0·56 ± 0.03 | 0·5465 |
| c Resolution of enthesitis (based on LEI) | 60·5 | 54·2 | 0·1498 |
| Exploratory | |||
| MDA | 43·0 | 37·9 | 0·1498 |
| VLDA | 18·1 | 16·6 | 0·6107 |
| DAPSA LDA+Remission | 61·7 | 53·1 | 0·0178 |
| PASDAS LDA+Remission | 51·1 | 44·1 | 0·0557 |
*Unadjusted P-values vs ADA
Binary variables were analysed using logistic regression. Pts who discontinued study treatment prematurely or took csDMARDs after week-36 were considered non-responders. Multiple imputation was used for all other missing data. HAQ-DI mean change from baseline was analysed using mixed-effect model repeated measures
a Non-responder imputation was used for pre-specified sensitivity analysis
b N=215 in SEC and N=202 in ADA in psoriasis subset
c N=234 in SEC and N=264 in ADA in enthesitis subset
Disclosure of Interests: Iain McInnes Grant/research support from: Bristol-Myers Squibb, Celgene, Eli Lilly and Company, Janssen, and UCB, Consultant of: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly and Company, Gilead, Janssen, Novartis, Pfizer, and UCB, Frank Behrens Grant/research support from: Pfizer, Janssen, Chugai, Celgene, Lilly and Roche, Consultant of: Pfizer, AbbVie, Sanofi, Lilly, Novartis, Genzyme, Boehringer, Janssen, MSD, Celgene, Roche and Chugai, Philip J Mease Grant/research support from: Abbott, Amgen, Biogen Idec, BMS, Celgene Corporation, Eli Lilly, Novartis, Pfizer, Sun Pharmaceutical, UCB – grant/research support, Consultant of: Abbott, Amgen, Biogen Idec, BMS, Celgene Corporation, Eli Lilly, Novartis, Pfizer, Sun Pharmaceutical, UCB – consultant, Speakers bureau: Abbott, Amgen, Biogen Idec, BMS, Eli Lilly, Genentech, Janssen, Pfizer, UCB – speakers bureau, Arthur Kavanaugh Grant/research support from: Abbott, Amgen, AstraZeneca, BMS, Celgene Corporation, Centocor-Janssen, Pfizer, Roche, UCB – grant/research support, Christopher T. Ritchlin Grant/research support from: UCB Pharma, AbbVie, Amgen, Consultant of: UCB Pharma, Amgen, AbbVie, Lilly, Pfizer, Novartis, Gilead, Janssen, Peter Nash Grant/research support from: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly and Company, Gilead, Janssen, MSD, Novartis, Pfizer Inc, Roche, Sanofi, UCB, Consultant of: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, Janssen, MSD, Novartis, Pfizer Inc, Roche, Sanofi, UCB, Speakers bureau: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, Janssen, MSD, Novartis, Pfizer Inc, Roche, Sanofi, UCB, Jordi Gratacos-Masmitja Grant/research support from: a grant from Pfizzer to study implementation of multidisciplinary units to manage PSA in SPAIN, Consultant of: Pfizzer, MSD, ABBVIE, Janssen, Amgen, BMS, Novartis, Lilly, Speakers bureau: Pfizzer, MSD, ABBVIE, Janssen, Amgen, BMS, Novartis, Lilly, Philippe Goupille Grant/research support from: AbbVie, Amgen, Biogen, BMS, Celgene, Chugai, Lilly, Janssen, Medac, MSD France, Nordic Pharma, Novartis, Pfizer, Sanofi and UCB, Consultant of: AbbVie, Amgen, Biogen, BMS, Celgene, Chugai, Lilly, Janssen, Medac, MSD France, Nordic Pharma, Novartis, Pfizer, Sanofi and UCB, Speakers bureau: AbbVie, Amgen, Biogen, BMS, Celgene, Chugai, Lilly, Janssen, Medac, MSD France, Nordic Pharma, Novartis, Pfizer, Sanofi and UCB, Tatiana Korotaeva Grant/research support from: Pfizer, Consultant of: Abbvie, BIOCAD, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, Merck Sharp & Dohme, Novartis, Novartis-Sandoz, Pfizer, UCB, Speakers bureau: Abbvie, BIOCAD, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, Merck Sharp & Dohme, Novartis, Novartis-Sandoz, Pfizer, UCB, Alice B Gottlieb Grant/research support from:: Research grants, consultation fees, or speaker honoraria for lectures from: Pfizer, AbbVie, BMS, Lilly, MSD, Novartis, Roche, Sanofi, Sandoz, Nordic, Celltrion and UCB., Consultant of:: Research grants, consultation fees, or speaker honoraria for lectures from: Pfizer, AbbVie, BMS, Lilly, MSD, Novartis, Roche, Sanofi, Sandoz, Nordic, Celltrion and UCB., Speakers bureau:: Research grants, consultation fees, or speaker honoraria for lectures from: Pfizer, AbbVie, BMS, Lilly, MSD, Novartis, Roche, Sanofi, Sandoz, Nordic, Celltrion and UCB., Ruvie Martin Shareholder of: Novartis, Employee of: Novartis, Kevin Ding Employee of: Novartis, Pascale Pellet Shareholder of: Novartis, Employee of: Novartis, Shephard Mpofu Shareholder of: Novartis, Employee of: Novartis, Luminita Pricop Shareholder of: Novartis, Employee of: Novartis