fetching data ... 
Background: Pneumococcal vaccinations are recommended for patients with rheumatoid arthritis (RA). There is evidence that pneumococcal vaccinations are less effective when administered after starting conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs). Vaccination guidelines have changed over time, since 1992 UK guidelines recommend pneumococcal vaccination for the immunocompromised, and in 2003 was expanded to all individual’s age ≥65 years. Guidelines from British Society of Rheumatology (2011) and EULAR (2019) advise to vaccinate prior to starting csDMARDs where possible. There is little evidence about whether these guidelines are being followed.
Objectives: The aims of this study were to explore the timing of pneumococcal vaccination in patients with RA in relation to starting csDMARDs and examine whether this has changed over time.
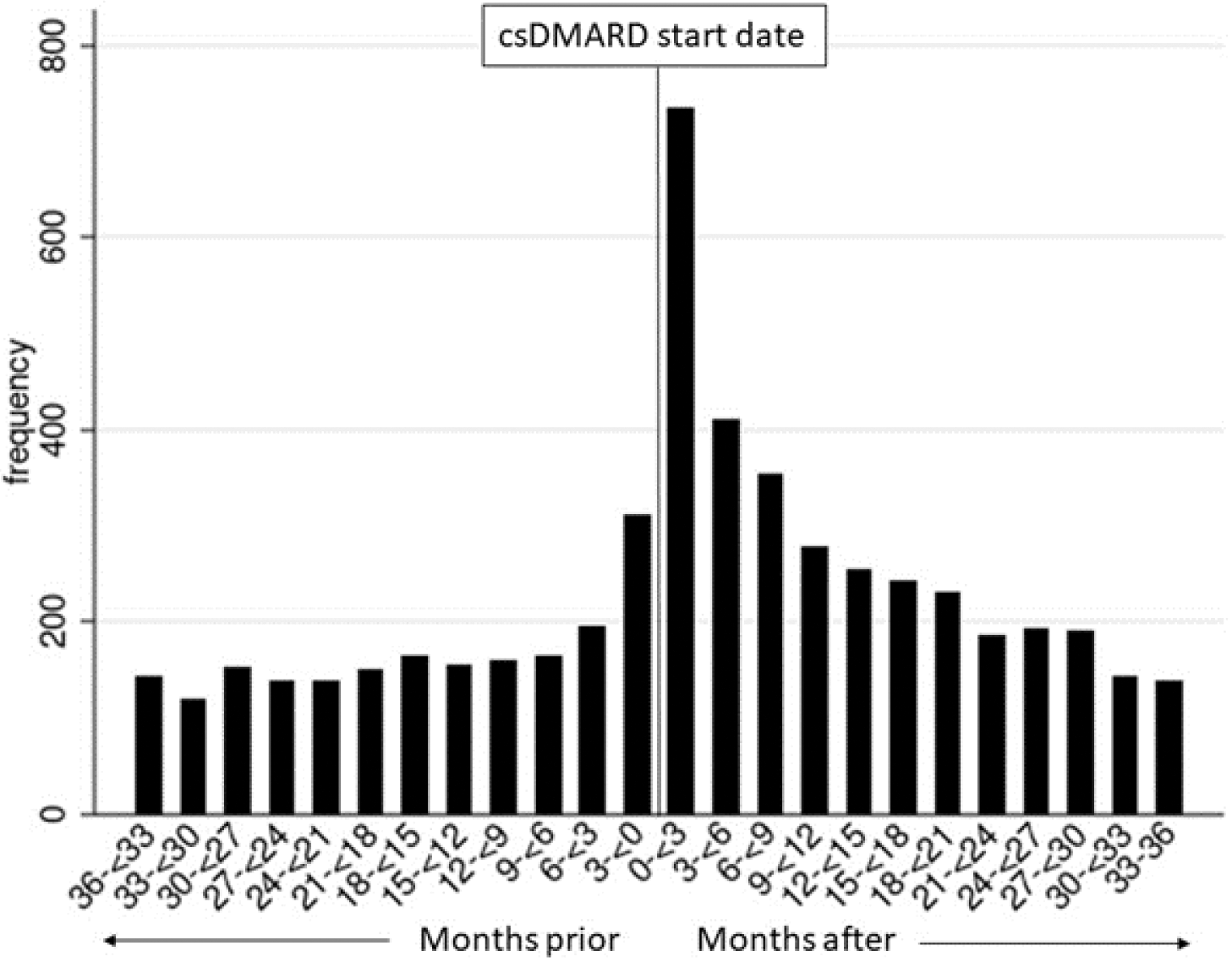
Methods: This was a cross-sectional study using UK electronic health records from primary care between 1st January 2000 and 31st December 2018. To be included in the study patients needed to 1) have a diagnosis of RA, 2) be prescribed csDMARDs up to 3 months prior to, or after RA diagnosis date and 3) have received a pneumococcal vaccination. Index date was considered the start of csDMARDs and vaccinations were required to be up to 5 years prior to the index date or after index date until leaving the practice, death or the end of the study period. For each patient it was determined if the first vaccination was prior to starting csDMARDs. For those vaccinated up to 3 years prior to, or up to 3 years after starting csDMARDs, the time between vaccination and starting csDMARDs in months was determined and this distribution was plotted in a bar chart. To explore how timing of vaccination has changed over time the proportion (with 95% confidence intervals (CI)) of people vaccinated prior to starting csDMARDs was plotted by year.
Results: Of 21461 people with RA identified who were prescribed their first csDMARD on or after 1st January 2000, there were 8205 (38.2%) patients vaccinated and eligible to be included in the study. The cohort had a mean age 62 years, 66.4% were female. There were 2997 (36.5%) patients vaccinated prior to starting csDMARDs. Those vaccinated prior to starting csDMARDs were older, with 72% (n=2168) being aged 65 years or over vs 28% (n=1465) in those vaccinated after starting csDMARDs. 5358 (65.3%) were vaccinated up to 3 years prior to, or up to 3 years after starting csDMARDs. The distribution showed that the most frequent time of vaccination was in the 3 months after starting csDMARDs and the frequency was higher in the months after starting csDMARDs than in the months preceding (
Time between starting csDMARDs and pneumococcal vaccination
Proportion and 95% confidence interval of those vaccinated prior to starting csDMARDs by year.
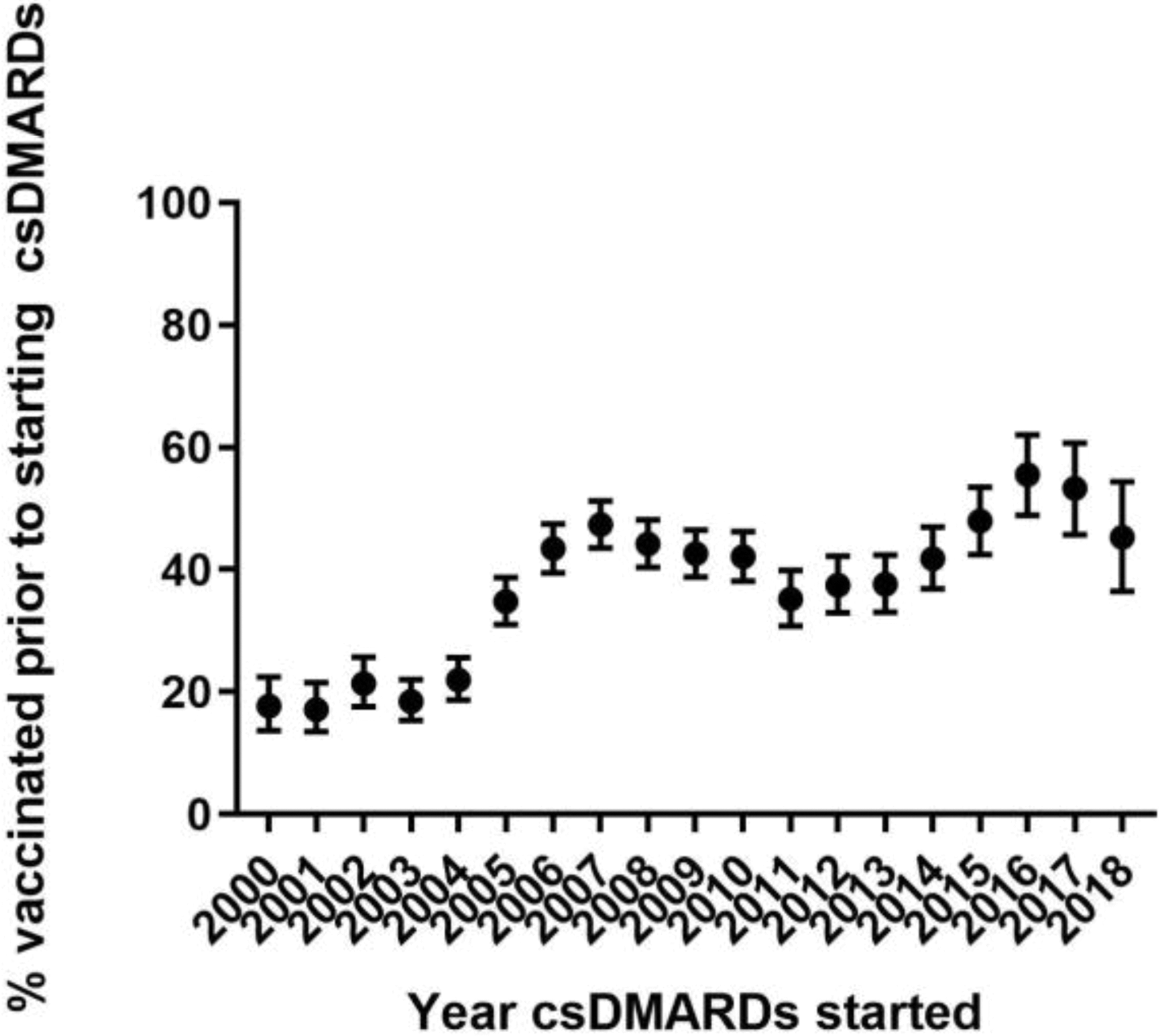
Conclusion: This study shows that timing of pneumococcal vaccination is improving with a trend towards increasing vaccination prior to starting csDMARDs and a high proportion of patients were vaccinated around the time of csDMARD initiation. However, just over a fifth (22.5%) were vaccinated more than 3 years after starting csDMARDs. Rheumatologists need to continue to work to raise awareness of the importance of vaccinations through better communications to patients and primary care physicians, to ensure best practice is being followed.
Disclosure of Interests: Ruth E Costello: None declared, Jenny Humphreys: None declared, Kevin Winthrop Grant/research support from: Bristol-Myers Squibb, Consultant of: AbbVie, Bristol-Myers Squibb, Eli Lilly, Galapagos, Gilead, GSK, Pfizer Inc, Roche, UCB, William Dixon Consultant of: Bayer and Google