fetching data ... 
Background: There is considerable debate regarding the most appropriate outcome measures for clinical trials in systemic lupus erythematosus (SLE). We propose that studying changes in disease activity over time may yield important information above and beyond fixed endpoints at 12 months.
Objectives: To compare outcomes and predictors of response using i) traditional response definitions at a fixed time point and ii) trajectories of disease activity over time in a clinical trial dataset.
Methods: Data from the phase 3 clinical trial of Epratuzumab (EMBODY) in patients with active SLE were reanalysed. Response at 12 months was defined as: reduction to ≤1 BILAG B score, no increase in SLEDAI-2K score and no increase in prednisolone dose. Latent class mixed models (LCMM) were constructed using the numerical BILAG-2004 (nBILAG) score (where A=12, B=8, C=1, D/E=0) from the screening visit until trial end. Cumulative prednisolone and Epratuzumab exposure was determined by estimating the area under the dose-time or concentration-time curves (AUC) respectively.
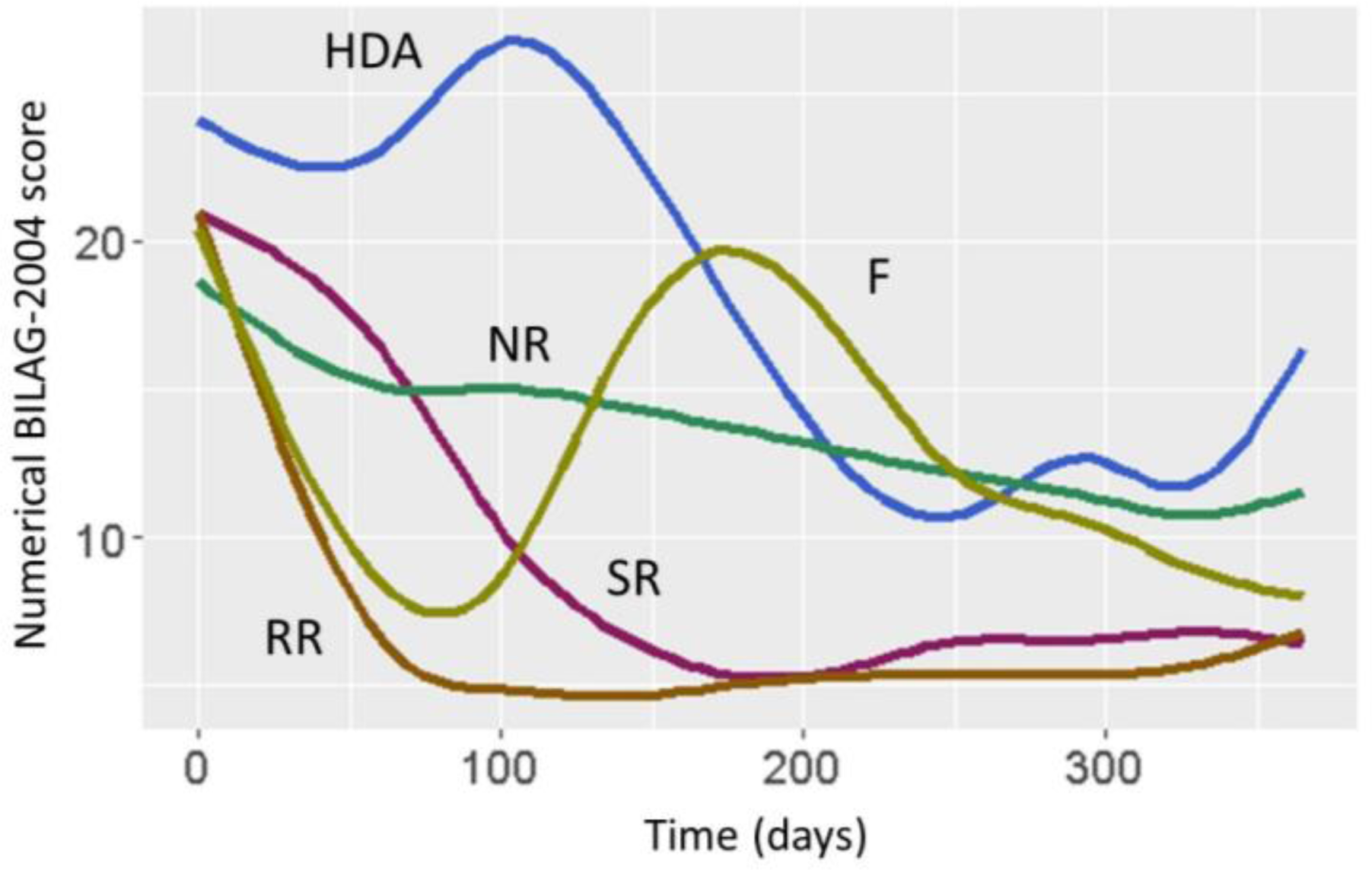
Results: 1202 patients were included with a median disease duration of 5.6 [1.9, 12.7] years and baseline nBILAG score of 20 [16, 24]. At 12 months there were 564/1202 (46.9%) responders. There was no association between receiving Epratuzumab and response. Responders were older, with lower baseline nBILAG score and baseline steroid dose. Using a cubic spline LCMM in the whole cohort, 5 trajectories were identified: Non-responders (NR, 33.9%), rapid responders (RR, 36.7%), slow responders (SR, 20.7%), flare (F, 4.7%) and high disease activity (HDA, 3.9%) (figure). Of the 564 12-month responders, 113 (20.4%) were in the NR latent class whilst 417 (73.9%) were in RR or SR classes. Whilst there were no differences in study drop-out due to adverse events, withdrawal due to inefficacy was 20.6% in NR compared to 8.4% in RR and 7.6% in SR.
In multivariable logistic regression models adjusted for age, gender and study drop-out, being a responder (RR or SR) was significantly associated with activity in constitutional, musculoskeletal and cardiorespiratory BILAG domains, higher baseline and cumulative steroid exposure, and receiving active drug.
There was a trend towards higher baseline CD19+ counts in RR compared to NR or SR (p=0.108) but in a population-averaged multivariable linear model only baseline CD19+ count, Epratuzumab and steroid dose were associated with number of CD19+ cell over time (p<0.001 for each).
Conclusion: Compared to a fixed end-point at 12 months, LCMM identified trajectories of disease activity and an association between clinical improvement and receiving active drug. Predictors of response vary significantly according to the response definition used.
Comparison of predictors of response between the 2 models
| Response at 12 months | Response latent call (RR or SR) | |
|---|---|---|
| Age | Yes | No |
| Baseline gBILAG score | Yes (negative) | Yes (positive) |
| Baseline steroid dose | Yes | Yes |
| Active disease | ||
| Constitutional | No | Yes |
| Musculoskeletal | No | Yes |
| Cardiorespiratory | No | Yes |
| Gastroenterological | Yes | No |
| Anti-Smith | Yes | No |
| Low C3 | Yes | No |
| Epratuzumab | No | Yes |
Acknowledgments: Presented on behalf of the MASTERPLANS Consortium
Disclosure of Interests: John Reynolds: None declared, Jennifer Prattley: None declared, Mark Lunt: None declared, Nophar Geifman: None declared, Ian N. Bruce Grant/research support from: Genzyme Sanofi, GSK, and UCB, Consultant of: Eli Lilly, AstraZeneca, UCB, Iltoo, and Merck Serono, Speakers bureau: UCB