fetching data ... 
Background: Clinical presentation of GCA is protean. It is vital to make a secure diagnosis, exclude mimics urgently and avoid inappropriate steroids to minimise side effects. Fast track GCA clinics (FTC) provide rapid specialist assessment with temporal and axillary US (1). EULAR recommendations support US as first-choice test. A pre-test probability score (PTPS) stratifies patients to low (LC), intermediate (IC) and high-risk (HC) categories.
Objectives: To validate a diagnostic GCA algorithm based on stratification by PTPS, with sequential US and additional tests (AT), if necessary
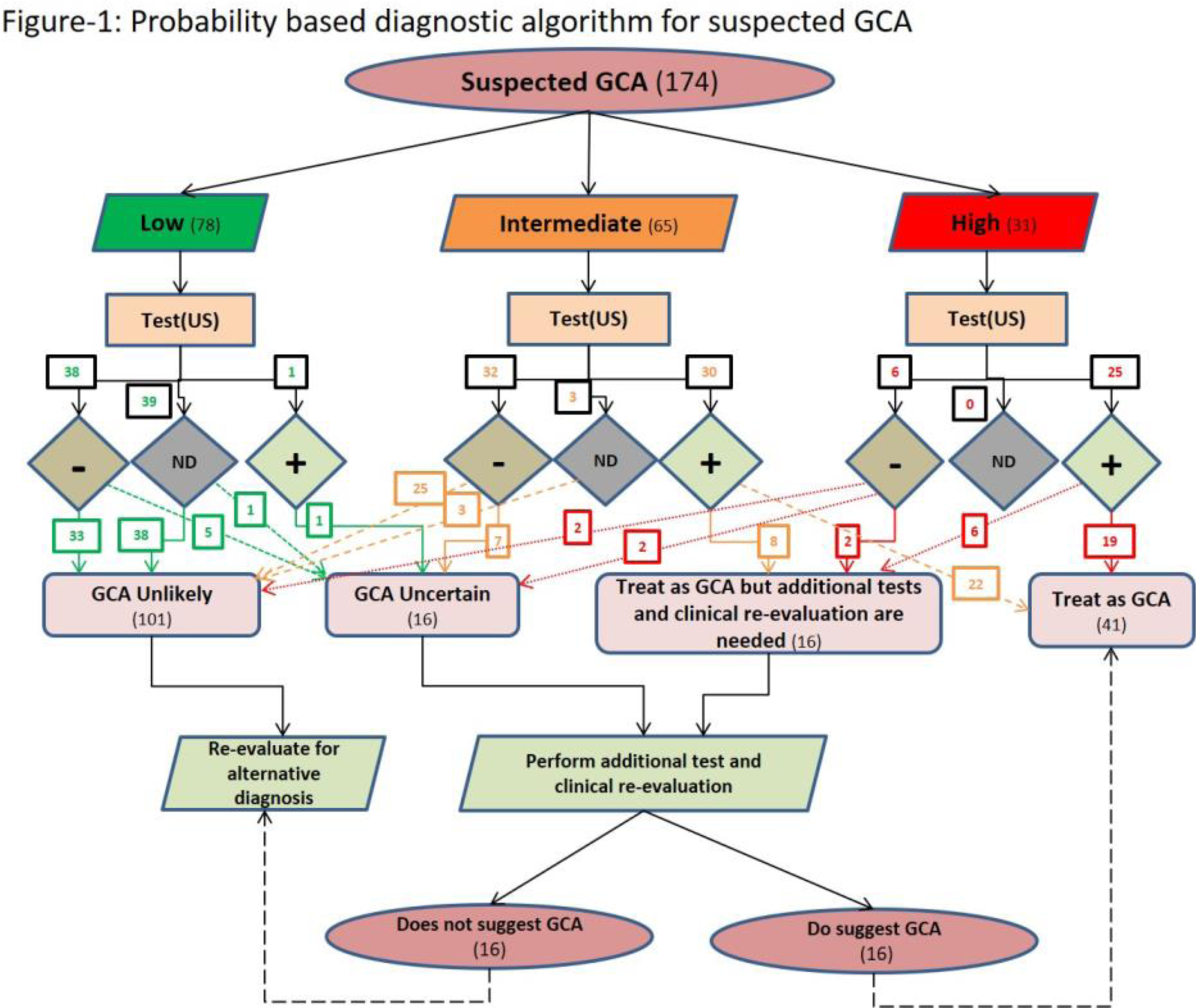
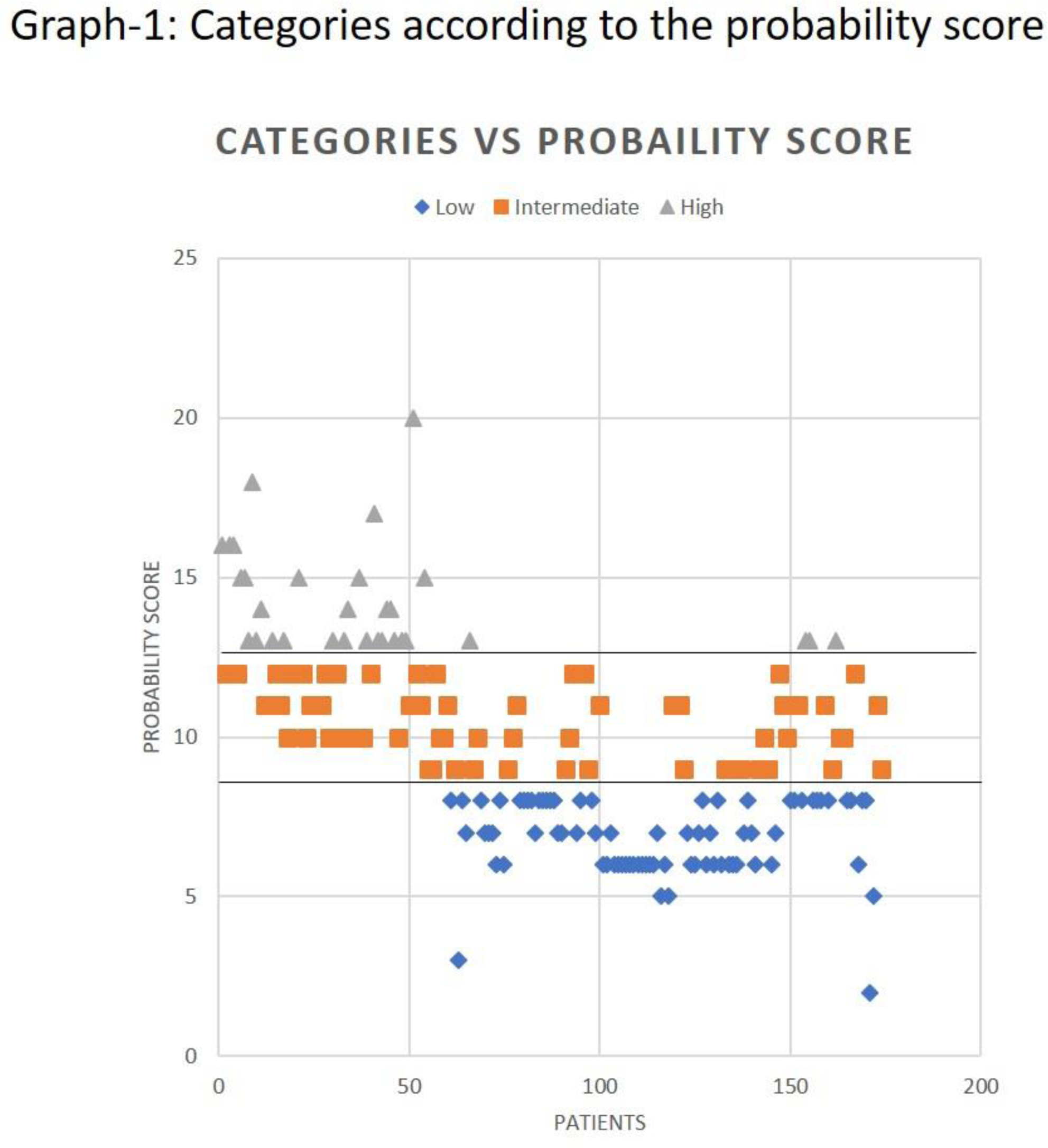
Methods: For the algorithm (Figure) retrospective data was extracted from case records of cases seen in 2019. PTPS overall showed median (Q2) score of 9,75 th percentile (Q3) score 12. Based on this and reported cut-off 9.5 (2) we classified LC as PTPS <9, IC 9-12 and HC >12 (Graph). GCA diagnosis was by modified GiACTA including US (Halo), CRP > 5 mg/L and AT if necessary. The algorithm performance was assessed overall and in individual categories.
Results: Of 187 consecutive cases, 13 were excluded for incomplete data (tertiary referrals). In remaining 174, GCA confirmed 33%, mean age 72.4 years, 69% females,45% LC, 35% IC, and 20% HC. 130 (75%) had US whereas 44 did not (41 LC, 3 IC) (Figure)
In HC, 25/31 (81%) were US +ve, 19 treated as GCA without AT, 6 with AT (
US performance with PTPS
|
Category
| US | GCA, n | Non-GCA, n | Sensitivity (% ) | Specificity (% ) | PPV (% ) |
NPV
| Prevalence (% ) |
Accuracy
|
|---|---|---|---|---|---|---|---|---|---|
| HC (31 ) | + | 24 | 1 | 24/27
| 3/4
| 24/25
| 3/6
| 27/31
| (24 + 3)/31
|
| - | 3 | 3 | |||||||
| IC (65 ) | + | 30 | 0 | 30/30
| 35/35
| 30/30
| 35/35
| 30/65
| (30 + 35)/65
|
| - | 0 | 35 | |||||||
| LC (78 ) | + | 0 | 1 | 0/0 (undefined) | 77/78
| 0/1
| 77/77
| 0/78
| (0 + 77)/78
|
| - | 0 | 77 | |||||||
| Total (174 ) | + | 54 | 2 | 54/57
| 115/117
| 54/56
| 115/118
| 57/174
| (54 + 115)/174
|
| - | 3 | 115 |
Abbreviations: GCA, Giant cell arteritis; NPV, Negative predictive value; PPV, Positive predictive value; US, Ultrasound
US, AT & confirmed diagnosis
| Category | Ultrasound | No of AT | Type of AT | Final Diagnosis | ||
|---|---|---|---|---|---|---|
| +ve | Not done | -ve | ||||
| LC (78) | 1 | 39 | 38 | 7 | 1x TAB (-), CTB (-) | Fibromyalgia |
| 1x TAB (-), MRA (-), MR neck (+) | Tongue cancer | |||||
| 1x CTA (+) | Stroke | |||||
| 1x CTCAP (-) | IA | |||||
| 1x PET (-) | PMR | |||||
| 1xTAB (-) | NA AION | |||||
| 1x PET (-) | CVA | |||||
| IC (65) | 30 | 3 | 32 | 15 | 5x TAB (-), 2x PET (-) | Not GCA |
| 2x TAB (+), 6x PET (+) | GCA | |||||
| HC (31) | 25 | 0 | 6 | 10 | 1x PET (-) | URTI |
| 1x TAB (-) | NAAION | |||||
| 2x PET (+) | ||||||
| 1x TAB (+) | ||||||
| 1x CTA (+) | ||||||
| 1x MRA (+) | GCA | |||||
| 1x PET (-) | ||||||
| 2x CTA (-) | ||||||
| 1x CTCAP (-) | ||||||
Abbreviations: AT, Additional test; CTA, Computed tomography angiogram; CTB, Computed tomography of brain; CTCAP, Computed tomography of chest, abdomen and pelvis; GCA, Giant cell arteritis; IA, Inflammatory arthritis; MRA, Magnetic resonant angiogram; NA AION, Non arteritic anterior ischemic optic neuritis; PET, Position emission tomography; TAB, Temporal artery biopsy; URTI, Upper respiratory tract infection
In LC, 38 (49%) were US - ve, of whom 5 had AT. US not done on 39 (50%) for either PTPS very low or urgent alternative diagnosis. 1 went on to AT. 1 was US positive and had GCA excluded with AT. US in LC showed specificity 99%, sensitivity 0/0 (undefined), accuracy 99%, GCA prevalence 0%, mean CRP 21.79 (SEM+/- 3.80)
In IC, 30/65 (46%) were US +ve 8 had AT (all GCA confirmed) while on treatment. 32 (49%) US negative where 7 had AT (all GCA excluded). 3 did not have US. Sensitivity, specificity, accuracy of US was all 100%, GCA prevalence 46%, mean CRP 39.05 (SEM+/- 5.04)
US test performance overall sensitivity 95%, specificity 98%, accuracy 97%
Conclusion: PTPS successfully stratifies GCA, excludes mimics and enhances US performance. The algorithm interprets correctly US findings and choice of AT.
REFERENCES:
[1]Patil et al Clin Exp Rheumatol 2015;33(Suppl 89): S103–6.
[2]Laskou et al. Clin Exp Rheumatol. 2019 Feb 15
Disclosure of Interests: Alwin Sebastian: None declared, Abdul Kayani: None declared, Chavini Ranasinghe: None declared, Bhaskar Dasgupta Grant/research support from: Roche, Consultant of: Roche, Sanofi, GSK, BMS, AbbVie, Speakers bureau: Roche