fetching data ... 
Background: Large numbers of patients with rheumatoid arthritis (RA) receive regular opioids despite significant toxicity and a lack of evidence supporting their use in non-cancer pain. In order to address this situation, we need to understand when opioids are started in early RA where this has not been studied.
Objectives: To examine the temporal trend of opioid prescriptions before and after RA symptom onset and to compare this with DMARD and NSAID prescriptions.
Methods: RA participants (cases) were recruited as part of the Scottish Early Rheumatoid Arthritis (SERA) inception cohort 1 . Controls without RA (five per case), matched for sex, age and post code over the same time period, were obtained through routine data linkage. Prescription data between Jan 2009 to Nov 2019 of cases and matched controls were compared using date of RA symptom onset as reference point. The Prescriptions Per Participant (PPP) for each three-month block was estimated by dividing the number of prescribed drugs in the selected drug classes (assigned using the British National Formulary) in that time block by the number of participants in each group. The differences between mean PPP of the RA cases and controls in each time block were tested by t-test for independent groups and subsequent adjustment for multiple testing.
Results: 1,720,335 prescriptions were available for analysis with 421,961 items for 950 RA cases and 1,299,374 items for 4,558 matched controls. As expected, DMARD prescriptions in the SERA cases increased after the symptom onset period and were then sustained (
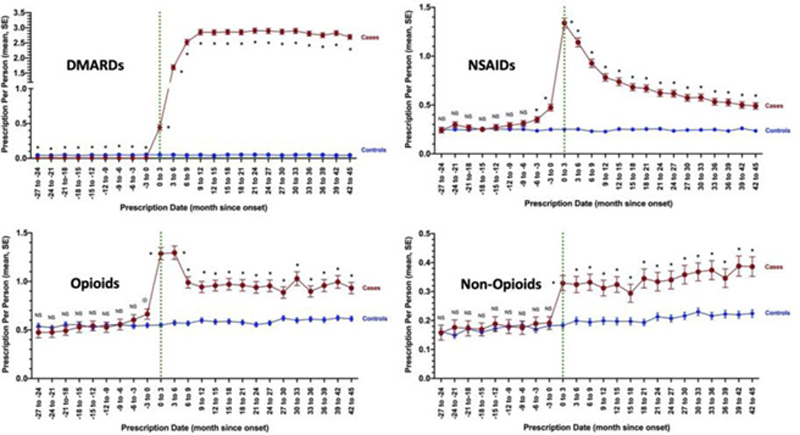
Conclusion: Opioid prescriptions increase significantly at the time of RA symptoms onset. Despite rapid introduction of DMARDs and resultant reductions in NSAIDs, analgesic use remains significantly higher than in controls. Further research is required to identify the factors associated with persistent opioid use in early RA with interventions aimed at the first 6 months.
REFERENCES:
[1]Dale et al. BMC Musculoskelet Disord. 2016;17:461.
Acknowledgements: The work was supported by Health Data Research UK which receives its funding from HDR UK Ltd funded by the UKRI MRC, EPSRC, Economic and Social Research Council, Department of Health and Social Care (England), Chief Scientists Office of the Scottish Government Health and Social Care Directorates, Health and Social Care Research and Development Division (Welsh Government), Public Health Agency (Northern Ireland), British Heart Foundation (BHF) and the Wellcome Trust.
The SERA study was jointly funded by the Chief Scientists Office Scotland and Pfizer Ltd.
Disclosure of Interests: None declared