fetching data ... 
Background: The EULAR recommendations for the management of systemic lupus erythematosus (SLE) suggest a hydroxychloroquine (HCQ) dose of ≤5.0 mg/kg/day instead of 6.5 mg/kg/day to reduce the risk of HCQ-induced retinopathy (1). This change in HCQ dose may potentially lead to undertreatment with blood levels below the presumed therapeutic range.
Objectives: The aim of this study was to compare flare rates and HCQ blood levels between the two different oral dosages in patients with SLE in remission.
Methods: Eligible patients were SLE patients in clinical remission according to the preliminary Definitions of Remission in SLE (DORIS) criteria for at least one year and treatment with stable dose of HCQ for at least six months and stable dose of glucocorticoids and/or immunosuppressants (2). Flares were defined by SELENA-SLEDAI Flare Index (3). A venous blood sample was collected on two different occasions from all patients, reflecting actual therapeutic adherence. The biosamples were analyzed in a UPLC-MS/MS system composed of a Nexera chromatograph (Shimadzu) coupled with a Q-trap 6500 spectrometer (AB Sciex). A mean [HCQ] value ([HCQm]) for each patient was then calculated. Predictors of flares were analyzed by Cox regression.
Results: We selected 66 patients who were stratified according to HCQ oral dose in two groups (
Conclusion: Our study suggests that low dosage of HCQ (5 mg/kg/day) may safely be prescribed in SLE patients in remission, without significant differences in terms of blood concentration and impact on the clinical course of SLE.
REFERENCES:
[1]Fanouriakis A, et al. Ann Rheum Dis 2019;78:736-745.
[2]van Vollenhoven R, et al. Ann Rheum Dis 2017;76:554-561.
[3]Petri M, et al. Arthritis Rheum. 2012;64(8):2677-2686.
Demographic, clinical and therapeutic features of the cohort and follow up data.
| All patients (n= 66) | HCQ
| HCQ
| P | |
| Sex, female | 65 (99) | 31 (97) | 34 (100) | 0,3026 |
| Age, y, mean (SD) | 42,00±11,27 | 41,80±10,25 | 42,10±12,30 | 0,9140 |
| Disease duration, y, mean (SD) | 15,70 (9,02) | 17,80 (8,01) | 13,67 (9,50) | 0,0624 |
| SLEDAI, median (range) | 2 (0-4) | 1 (0-4) | 2 (0-4) | 0,6480 |
| SLICC, median (range) | 0 (0-2) | 0 (0-2) | 0 (0-1) | 0,8556 |
| [HCQm] ng/mL, median (range) | 512,60
| 457,16
| 538,49
| 0,5989 |
| [DCQ] ng/mL,median (range) | 73,41
| 66,84
| 66,31
| 0,9380 |
| Time remission, y, median (range) | 2,00 (1-11) | 2,96 (1-10) | 2,00 (1-11) | 0,6588 |
| Previous renal involvement | 31 (47) | 15 (47) | 16 (47) | 0,9882 |
| Time HCQ, y, median (range) | 5 (0-32) | 8 (0-26) | 5 (1-32) | 0,2391 |
| Glucocorticoids | 33 (50) | 18 (56) | 15 (44) | 0,4700 |
| Mycophenolate mofetil | 6 (9) | 2 (6) | 4 (12) | 0,4396 |
| Azathioprine | 7 (11) | 4 (14) | 3 (9) | 0,6305 |
| Methotrexate | 1 (2) | 0 | 1 (3) | 0,3320 |
| Cyclosporine | 2 (3) | 1 (3) | 1 (3) | 0,9655 |
| Belimumab | 1 (2) | 0 | 1 (3) | 0,3320 |
| Follow up time, m, median (range) | 49 (4-67) | 52 (7-67) | 43 (4-67) | 0,1115 |
| Number of flares | 23 (35) | 8 (25) | 15 (44) | 0,1060 |
| Time to flare, m, mean (SD) | 26,0 (±15,1) | 26,6 (±16,4) | 25,8 (±14,9) | 0,9042 |
| Ocular alterations | 6 (9) | 4 (12) | 2 (6) | 0,0947 |
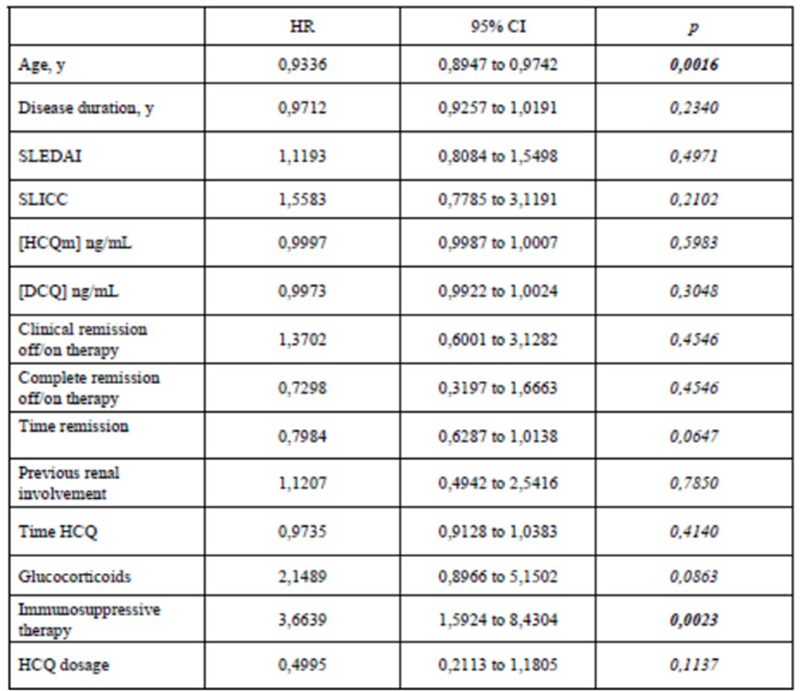
Predictors of flares analyzed by Cox regression. *Serena Fasano and Valentina Messiniti contributed equally to this abstract
Disclosure of Interests: None declared