fetching data ... 
Background: Although most patients with psoriatic arthritis (PsA) enrolled in clinical trials have polyarticular arthritis, patients in clinical practice may present with oligoarthritis. Data on the efficacy of Janus kinase inhibitors in patients with PsA with low joint counts are limited.
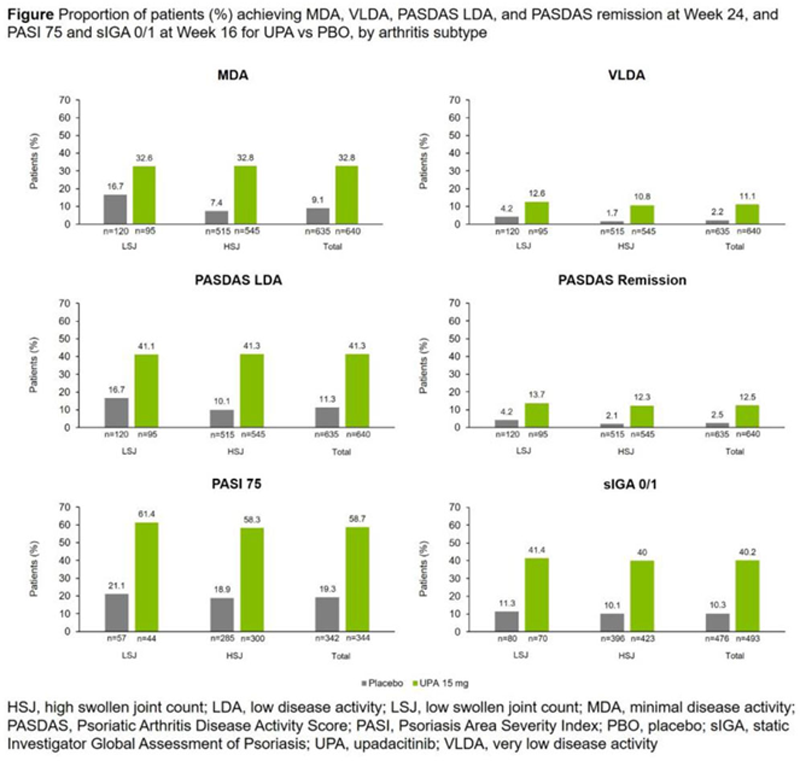
Objectives: To evaluate the efficacy of upadacitinib (UPA) in subgroups of patients with PsA with a low (baseline swollen joint count [SJC] <5) or high (SJC ≥5) SJC (LSJ or HSJ).
Methods: Data were pooled across the SELECT-PsA 1 1 (non-biologic disease-modifying antirheumatic drug [non-bDMARD] inadequate response [IR] or intolerance) and SELECT-PsA 2 2 (bDMARD IR or intolerance) trials, which both enrolled patients with ≥3 involved joints (SJC ≥3 and tender joint count [TJC] ≥3). Subgroup analysis was performed for patients with LSJ or HSJ treated with UPA 15 mg once daily (QD) or placebo (PBO). Efficacy endpoints included minimal disease activity (MDA), very low disease activity (VLDA), Psoriatic Arthritis Disease Activity Score (PASDAS) low disease activity (LDA; ≤3.2), PASDAS remission (≤1.9), and 20/50/70% improvement in American College of Rheumatology (ACR) criteria (ACR20/50/70), all at Week 24, and Psoriasis Area Severity Index (PASI) 75 and static Investigator Global Assessment of Psoriasis (sIGA) 0/1 at Week 16.
Results: At baseline, patients with HSJ (n=1060) had similar demographic characteristics but tended to have higher overall disease activity than patients with LSJ across multiple disease domains (n=215;
Baseline characteristics
| PBO | UPA 15 mg QD | Total | ||||
|
LSJ
|
HSJ
|
LSJ
|
HSJ
|
LSJ
|
HSJ
|
|
| Female, n (%) | 65 (54.2) | 266 (51.7) | 49 (51.6) | 302 (55.4) | 114 (53.0) | 568 (53.6) |
| Age (years), mean (SD) | 52.2 (12.7) | 51.5 (12.0) | 52.0 (10.6) | 52.0 (12.4) | 52.1 (11.8) | 51.8 (12.2) |
| Duration since PsA symptoms (years), mean (SD) | 10.5 (9.2) | 11.1 (10.2) | 9.8 (8.2) | 10.3 (8.9) | 10.2 (8.7) | 10.7 (9.6) |
| BMI, mean (SD) | 29.7 (6.3) | 31.1 (7.2) | 29.8 (6.2) | 30.7 (6.9) | 29.7 (6.2) | 30.9 (7.0) |
| Prior failed bDMARDs, n (%) | ||||||
| 0 | 3 (2.5) | 15 (2.9) | 1 (1.1) | 15 (2.8) | 4 (1.9) | 30 (2.8) |
| 1 | 22 (18.3) | 113 (21.9) | 22 (23.2) | 104 (19.1) | 44 (20.5) | 217 (20.5) |
| 2 | 4 (3.3) | 31 (6.0) | 7 (7.4) | 28 (5.1) | 11 (5.1) | 59 (5.6) |
| ≥3 | 4 (3.3) | 20 (3.9) | 7 (7.4) | 27 (5.0) | 11 (5.1) | 47 (4.4) |
| Use of ≥1 non-bDMARD at
| 87 (72.5) | 360 (69.9) | 63 (66.3) | 388 (71.2) | 150 (69.8) | 748 (70.6) |
| Dactylitis (LDI >0), n (%) | 21 (17.5) | 169 (32.8) | 15 (15.8) | 176 (32.3) | 36 (16.7) | 345 (32.5) |
| Enthesitis (LEI >0), n (%) | 60 (50.0) | 325 (63.1) | 60 (63.2) | 343 (62.9) | 120 (55.8) | 668 (63.0) |
| TJC68, mean (SD) | 12.5 (11.3) | 23.9 (15.8) | 14.6 (13.5) | 23.1 (15.8) | 13.4 (12.3) | 23.5 (15.8) |
| SJC66, mean (SD) | 3.5 (0.5) | 13.2 (8.3) | 3.6 (0.5) | 12.9 (9.0) | 3.6 (0.5) | 13.0 (8.7) |
| HAQ-DI, mean (SD) | 1.0 (0.6) | 1.2 (0.7) | 0.9 (0.6) | 1.2 (0.6) | 0.9 (0.6) | 1.2 (0.7) |
| hs-CRP > ULN (mg/L), n (%) | 82 (68.3) | 363 (70.5) | 62 (65.3) | 388 (71.2) | 144 (67.0) | 751 (70.8) |
| BSA-Ps, median (range) | 3.0 (0.1–70.0) | 4.0 (0.1–95.0) | 2.0 (0.1–80.0) | 3.0 (0.1–97.0) | 3.0 (0.1–80.0) | 3.0 (0.1–97.0) |
| BSA-Ps ≥ 3%, n (%) | 57 (47.5) | 285 (55.3) | 44 (46.3) | 300 (55.0) | 101 (47.0) | 585 (55.2) |
| PASI (baseline BSA-Ps ≥ 3%), mean (SD) | 7.7 (7.5) | 12.1 (11.9) | 8.2 (7.0) | 10.2 (10.0) | 7.9 (7.2) | 11.1 (11.0) |
| PASI (baseline BSA-Ps ≥ 3%), median (range) | 5.3 (0.1–39.4) | 7.9 (0.3–64.8) | 6.5 (0.2–35.4) | 6.8 (0.1–70.8) | 6.0 (0.1–39.4) | 7.3 (0.1–70.8) |
Conclusion: UPA efficacy was generally similar in patients with PsA with LSJ or HSJ, with both patient groups showing improvements in composite clinical endpoints and skin responses vs PBO.
REFERENCES:
[1]McInnes I, et al. Ann Rheum Dis 2020;79(Suppl. 1):16–17;
[2]Mease PJ, et al. Ann Rheum Dis 2020; Epub ahead of print.
Acknowledgements: AbbVie funded this study; contributed to its design; participated in data collection, analysis, and interpretation of the data; and participated in the writing, review, and approval of the abstract. No honoraria or payments were made for authorship. Medical writing support was provided by Grant Kirkpatrick, MSc of 2 the Nth (Cheshire, UK), and was funded by AbbVie.
Disclosure of Interests: Laure Gossec Consultant of: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, MSD, Novartis, Pfizer, Roche, Sanofi, and UCB, Grant/research support from: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, MSD, Novartis, Pfizer, Roche, Sanofi, and UCB, Dafna D Gladman Consultant of: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Amgen, Celgene, Eli Lilly, Novartis, Pfizer, and UCB, Erin McDearmon-Blondell Shareholder of: May own stock or options in AbbVie, Employee of: AbbVie, Philipp Sewerin Consultant of: AbbVie, Amgen, Axiom Health, Biogen, Bristol-Myers Squibb, Celgene, Chugai, Deutscher Psoriasis Bund, Eli Lilly, Fresenius Kabi, Gilead, Hexal, Janssen, Johnson & Johnson, Medi-login, Mediri, Novartis, Onkowissen, Pfizer, Roche, Rheumazentrum Rhein-Ruhr, Sanofi, Swedish Orphan Biovitrum, and UCB, Grant/research support from: AbbVie, Amgen, Biogen, Bristol-Myers Squibb, Bundesministerium fuer Bildung und Forschung, Deutsche Forschungsgesellschaft, Deutscher Psoriasis Bund, Eli Lilly, Fresenius Kabi, Gilead, Hexal, Janssen, Novartis, Pfizer, Rheumazentrum Rhein-Ruhr, Roche, Sanofi, and UCB, Christopher T. Ritchlin Consultant of: AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, Sun, and UCB, Grant/research support from: AbbVie, Amgen, and UCB, Dai Feng Shareholder of: May own stock or options in AbbVie, Employee of: AbbVie, Apinya Lertratanakul Shareholder of: May own stock or options in AbbVie, Employee of: AbbVie, R Ranza Consultant of: AbbVie, Eli Lilly, Janssen, Novartis, and Pfizer, Grant/research support from: AbbVie, Janssen, Novartis, and Pfizer, Lai-Shan Tam Consultant of: AbbVie, Boehringer Ingelheim, Eli Lilly, Janssen, Pfizer, and Sanofi, Grant/research support from: Amgen, Boehringer Ingelheim, GSK, Janssen, Novartis, and Pfizer, Antonio Marchesoni Consultant of: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, MSD, Novartis, Pfizer, and UCB, Laura C Coates: None declared., Peter Nash Consultant of: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, Janssen, MSD, Novartis, Pfizer, Roche, Sanofi, and UCB, Grant/research support from: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, Janssen, MSD, Novartis, Pfizer, Roche, Sanofi, and UCB.