fetching data ... 
Background: The Janus kinase (JAK)-1 preferential inhibitor filgotinib (FIL) improved rheumatoid arthritis (RA) signs and symptoms in 3 phase (P)3 trials. 1–3 Like other RA therapies, JAK inhibition is associated with increased infection rates. 4
Objectives: To assess long-term safety across the FIL program regarding infections, including serious infections (SI).
Methods: Patients (pts) meeting 2010 ACR/EULAR RA criteria in pooled analysis of P2 DARWIN 1–2 (D1–2), P3 FINCH 1–3 (F1–3), and long-term extension studies (DARWIN 3, FINCH 4) were included. The placebo (PBO)-controlled as-randomised data set included pts receiving FIL 100 mg (FIL100), FIL 200 mg (FIL200), or PBO up to week (W)12 (D1–2, F1–2). The active-controlled as-randomised data set included pts receiving FIL100, FIL200, adalimumab (ADA), or methotrexate (MTX) up to W52 (F1, F3). The long-term as-treated data set included pts in all 7 studies receiving FIL100 or FIL200; data after rerandomisation were included and contributed to treatment received.
Exposure-adjusted incidence rates (EAIRs) per 100 patient-years exposure (PYE) and differences with 95% confidence intervals (CIs) were calculated using Poisson regression; EAIRs for tuberculosis (TB) in active controlled sets were calculated using an Exact Poisson method. Kaplan-Meier (KM) event probabilities with 95% CIs were provided for SI. If pts had multiple events within the same treatment period, only the first event was counted in EAIR calculation; PYE were calculated up to the last follow-up time or day before next treatment, including after first event. For KM analysis, time to event was calculated until the first event.
Results: Of 2267/1647 pts in as-treated set receiving FIL200/FIL100, 1697 had treatment-emergent infection; 118 were SI. Baseline potential risk factors for pts with SI are in
Baseline characteristics of pts with/without treatment emergent SI a
| Parameter, n (% ) |
SI
|
No SI
|
| Medical history | ||
| Chronic lung disease | 13 (14.1) | 125 (5.0) |
| Chronic renal disease | 3 (3.3) | 23 (0.9) |
| Infections and infestations | 29 (31.5) | 499 (20.0) |
| Baseline body mass index, kg/m 2 | ||
| <30 | 64 (69.6) | 1749 (70.2) |
| ≥30 | 28 (30.4) | 742 (29.8) |
| Age, years | ||
| <65 | 67 (72.8) | 2006 (80.5) |
| ≥65 | 25 (27.2) | 485 (19.5) |
| Former/current smoker | 30 (32.6) | 677 (27.2) |
| Oral corticosteroids, mg | ||
| <7.5 | 28 (56.0) | 731 (66.1) |
| ≥7.5 | 22 (44.0) | 375 (33.9) |
| Missing data | 42 | 1385 |
a Phase 3 (FINCH 1-4) studies, as randomised.
SI, serious infection.
In 12W PBO-controlled period, infection rates were 17.9%/15.6%/13.3% for FIL200/FIL100/PBO. In 52W ADA-controlled period, infection EAIRs (95% CIs)/100 PYE were 46.9 (40.9, 53.7)/43.7 (38.0, 50.4)/43.4 (36.5, 51.5), FIL200/FIL100/ADA; and 38.5 (33.8, 43.9)/39.0 (31.1, 48.8)/42.2 (36.1, 49.3), FIL200/FIL100/MTX in 52W MTX-controlled period; 24.8 (23.1, 26.5)/34.4 (30.4, 38.8), FIL200/FIL100 in long-term analysis. In 12W PBO-controlled period, there was no active TB for FIL200/FIL100/PBO. In 52W ADA-controlled period, active TB EAIRs (95% CIs)/100 PYE were: 0 (0.0, 0.8)/0 (0.0, 0.8)/0.3 (0.0, 1.9), FIL200/FIL100/ADA and 0 (0.0, 0.6)/0 (0.0, 1.9)/0 (0.0, 1.0), FIL200/FIL100/MTX in 52W MTX-controlled period; 0/0.1 (0.0, 0.5), FIL200/FIL100 in long-term analysis.
SI rate or EAIRs are in
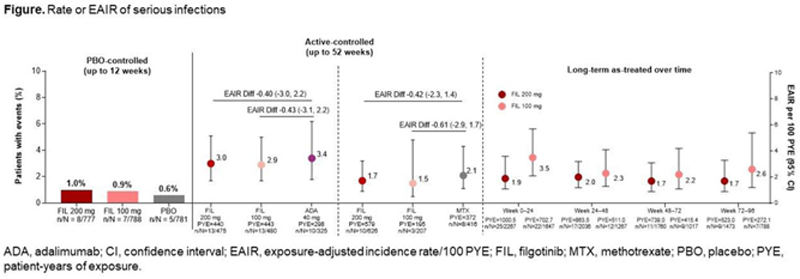
Conclusion: EAIRs of infections and SI for FIL were similar to PBO, ADA, and MTX. At 52W, incidence rates of SI were comparable for FIL100 and FIL200. Long-term SI EAIR for FIL100 was slightly higher than for FIL200.
REFERENCES:
[1]Genovese et al. JAMA . 2019;322:315–25.
[2]Westhovens et al. Ann Rheum Dis . 2021; online first.
[3]Combe et al. Ann Rheum Dis . 2021; online first.
[4]Strand et al. Arthritis Res Ther. 2015;17:362.
Disclosure of Interests: James Galloway Speakers bureau: Pfizer, Bristol-Myers Squibb, UCB and Celgene, Maya H Buch Consultant of: Pfizer; AbbVie; Eli Lilly; Gilead Sciences, Inc.; Merck-Serono; Sandoz; and Sanofi, Grant/research support from: Pfizer, Roche, and UCB, Kunihiro Yamaoka Speakers bureau: AbbVie, Actelion Pharmaceuticals Japan, Asahikasei Pharma Corp, Astellas Pharma, AYUMI Pharma Co, Boehringer Ingelheim Japan, Bristol-Myers Squibb, Chugai Pharma, Daiichi Sankyo, Eisai Pharma, Eli Lilly, GlaxoSmithKline, Gilead G.K., Hisamitsu Pharma Co., Janssen Pharma, Mitsubishi-Tanabe Pharma, MSD, Nippon Kayaku, Nippon Shinyaku, Ono Pharma, Otsuka Pharma, Pfizer, Sanofi, and Takeda Industrial Pharma, Consultant of: Asahikasei Pharma Corp., AbbVie, Gilead G.K., Pfizer, Astellas Pharma Inc, Eli Lilly Japan K.K., and Japan Tobacco Inc., Grant/research support from: Takeda Industrial Pharma, Pfizer, Astellas Pharma, Daiichi Sankyo, Eli Lilly, Eisai Pharma, Teijin Pharma, MSD, Shionogi, Chugai Pharma, Nippon Kayaku, Mitsubishi-Tanabe Pharma, and AbbVie, Cianna Leatherwood Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Alena Pechonkina Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Iyabode Tiamiyu Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Deyuan Jiang Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Lei Ye Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Robin Besuyen Shareholder of: Galapagos BV, Employee of: Galapagos BV, Daniel Aletaha Speakers bureau: AbbVie, Celgene, Lilly, Merck, Novartis, Pfizer, Sanofi Genzyme, UCB, Consultant of: AbbVie, Amgen, Celgene, Lilly, Medac, Merck, Novartis, Pfizer, Roche, Sandoz, Sanofi Genzyme, Grant/research support from: AbbVie, Novartis, Roche, Kevin Winthrop Consultant of: AbbVie, Bristol-Myers Squibb, Eli Lilly and Co., Galapagos NV, Gilead Sciences, GlaxoSmithKline, Pfizer, Roche, and UCB, Grant/research support from: AbbVie, Bristol-Myers Squibb, and Pfizer