fetching data ... 
Background: Several large randomised controlled trials (RCTs) in primary Sjögren’s syndrome (pSS) failed to demonstrate drug efficacy. 1-4 Many of these trials used ESSDAI as primary endpoint, showing large but similar response rates in active treatment and placebo groups. 1,3,4 Given the heterogeneous nature of pSS, there is need for a composite endpoint including multiple clinically relevant parameters.
Objectives: To develop and validate the Composite of Relevant Endpoints in Sjögren’s Syndrome (CRESS).
Methods: A multidisciplinary team of pSS experts selected clinically relevant items and measurements to include in the CRESS. Definition of response of CRESS items was based on clinical relevance, previously defined minimal clinically important improvement (MCII) and data of the single-centre ASAP-III (abatacept) trial. 1 CRESS was validated in three independent RCTs: TRACTISS (rituximab) trial 2 , multi-centre abatacept trial 3 and ETAP (tocilizumab) trial 4 . CRESS response rates were assessed at the primary endpoint visit of all four trials.
Results: Five complementary items were selected to form CRESS: systemic disease activity, patient-reported symptoms, tear gland, salivary gland and serological item. Definition of response per item is presented in
CRESS items and definition of response
| Items | Measurements | Definition of response |
| Systemic disease activity | ClinESSDAI | Score<5 (low disease activity) |
| Patient-reported symptoms | ESSPRI | Decrease of ≥1 point or ≥15% |
| Tear gland* | Schirmer/OSS** | -If abnormal Schirmer (≤5 mm) at baseline: increase of ≥5 mm in Schirmer |
| -Or if abnormal OSS (≥3 points) at baseline: decrease ≥2 points in OSS | ||
| -Or if both Schirmer/OSS normal scores at baseline: no change to abnormal in both | ||
| Salivary gland* | UWS/SGUS | Increase of ≥25% in UWS (or if score is 0 at baseline, any increase) |
| Or decrease of ≥25% in total Hocevar score (SGUS) | ||
| Serological | RF/IgG | Decrease of ≥25% in RFOr decrease of ≥10% in IgG |
| CRESS responder | Responder on ≥3 of 5 items | |
Ocular Staining Score (OSS), Unstimulated whole salivary flow (UWS), Salivary gland ultrasonography (SGUS), Rheumatoid factor (RF), Immunoglobuline G (IgG)
*Concise CRESS (cCRESS): CRESS without OSS and SGUS, leaving Schirmer and UWS for tear and salivary gland items, respectively
**Mean of both eyes
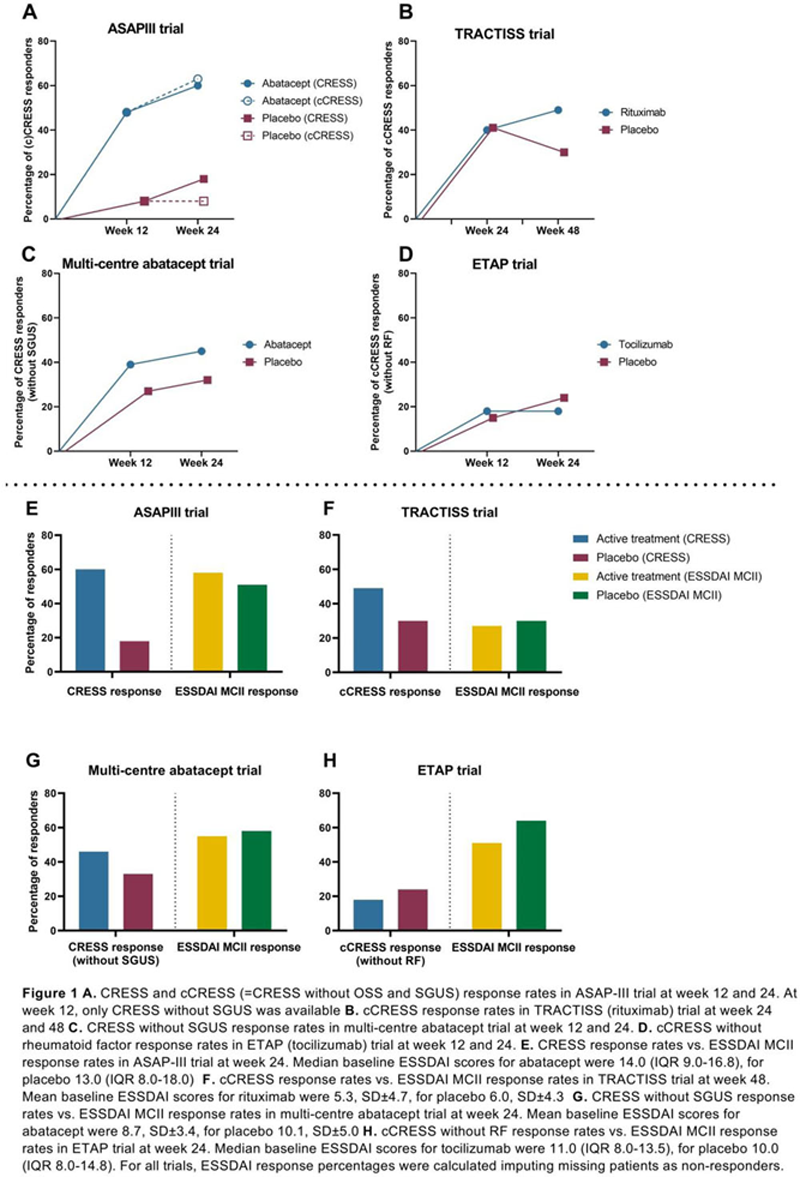
In the external validation trials, cCRESS response rates for TRACTISS were: 33/67 (49%) rituximab vs. 20/66 (30%) placebo at week 48 (p=0.026). CRESS response rates (without SGUS) for the multi-centre abatacept trial were: 41/92 (45%) abatacept vs. 30/95 (32%) placebo at week 24 (p=0.067). cCRESS response rates (without rheumatoid factor) for ETAP were: 10/55 (18%) tocilizumab vs. 13/55 (24%) placebo at week 24 (p=0.482) (
Conclusion: CRESS shows lower placebo response rates compared to ESSDAI MCII, which is crucial for demonstrating treatment efficacy. With the CRESS, higher response rates in abatacept and rituximab treated patients compared to placebo were found in RCTs which previously showed negative primary endpoint results. CRESS confirmed that no differences were found for almost all outcome measures between tocilizumab and placebo, 4 with low response rates. The CRESS is a well-balanced, feasible, composite endpoint for use in clinical trials in pSS patients.
REFERENCES:
[1]Van Nimwegen 2020;9913(19):1–11
[2]Bowman 2017;69(7):1440–50
[3]Baer (doi:218599)
[4]Felten (doi:21846)
Acknowledgements: The authors would like to acknowledge all contributors of the included trials.
Disclosure of Interests: Suzanne Arends: None declared, Liseth de Wolff: None declared, Jolien F. van Nimwegen Speakers bureau: Bristol Myers Squibb, Consultant of: Bristol Myers Squibb, Gwenny M. Verstappen: None declared, Jelle Vehof: None declared, Michele Bombardieri Consultant of: MedImmune, GlaxoSmithKline, Grant/research support from: MedImmune, Simon J. Bowman Consultant of: AstraZenecea/MedImmune, Bristol Myers Squibb, Celgene, Eli Lilly, Glenmark, GlaxoSmithKline, MTPharma, Novartis, Ono, Pfizer, Takeda, UCB, XTLBio, Elena Pontarini: None declared, Alan Baer Consultant of: Bristol Myers Squibb, Sanofi, VielaBio, Novartis, Marleen Nys Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Jacques-Eric Gottenberg Grant/research support from: Bristol Myers Squibb, Pfizer, Renaud FELTEN: None declared, Neelanjana Ray Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Arjan Vissink: None declared, Frans G.M. Kroese Speakers bureau: Bristol Myers Squibb, Roche and Janssen-Cilag, Consultant of: Bristol Myers Squibb, Grant/research support from: Unrestricted grants from Bristol Myers Squibb, Hendrika Bootsma Speakers bureau: Bristol Myers Squibb and Novartis, Consultant of: Bristol Myers Squibb, Roche, Novartis, Medimmune, Union Chimique Belge, Grant/research support from: Unrestricted grants from Bristol Myers Squibb and Roche