fetching data ... 
Background: Up to 50% of patients with RA discontinue DMARD treatment within 18 months. 1 However, up to 20% of patients who fail multiple treatments may have a good treatment response to another therapy. 1 Predictive biomarkers, such as RF and anti-citrullinated protein antibodies (ACPAs), may be useful to stratify patients with RA to the most appropriate treatment. 1 ASCORE ( A batacept S ub C utane O us in R outine Clinical Practic E ; NCT02090556) was a 2-year, observational, prospective, multicentre study of SC abatacept for the treatment of RA in routine clinical practice. 2
Objectives: To determine if RF/ACPA serostatus and treatment line impact abatacept retention in patients with RA in a post hoc analysis of ASCORE.
Methods: Eligible patients, aged ≥18 years, with active moderate-to-severe RA (ACR/EULAR 2010 criteria) who were IV abatacept-naive and initiated SC abatacept 125 mg once weekly, were enrolled into two cohorts: biologic (b)DMARD-naive patients and those with ≥1 prior bDMARD treatment failure. This post hoc analysis assessed abatacept retention rate at 2 years in a subset of patients with RF/ACPA serostatus data (n=1748) from the ASCORE study (N=2892; as observed). Baseline (BL) serostatus groups examined by treatment line were: RF/ACPA double positive (+/+) RA, RF/ACPA single positive (RF+/ACPA– or RF–/ACPA+) RA (data not shown) and RF/ACPA double negative (–/–) RA. Last observation carried forward (LOCF) analyses were used to assess change from BL and measures of disease remission (DAS28 [CRP] <2.6, CDAI ≤2.8, and SDAI ≤3.3) in patients with +/+ RA versus –/– RA.
Results: BL demographic and disease characteristics were similar across serostatus groups and treatment lines (
BL demographics and disease characteristics by RF/ACPA status
|
+/+ RA
|
–/– RA
|
|||
| First-line (n=511 ) | ≥ second-line (n=568 ) |
First-line
|
≥ second-line
|
|
| Age | 57.1 (13.4) | 57.1 (12.2) | 59.5 (14.7) | 56.6 (13.2) |
| DAS28 (CRP ) | 4.7 (1.2) | 4.7 (1.2) | 4.8 (1.1) | 4.8 (1.2) |
| CDAI | 26.6 (12.5) | 26.6 (12.4) | 27.7 (12.5) | 28.6 (13.8) |
| SDAI | 28.1 (13.1) | 28.1 (12.9) | 29.1 (12.9) | 30.2 (14.7) |
Data are mean (SD). Patients with missing data for BL RF/ACPA status are excluded.
ACPA=anti-citrullinated protein antibody; BL=baseline.
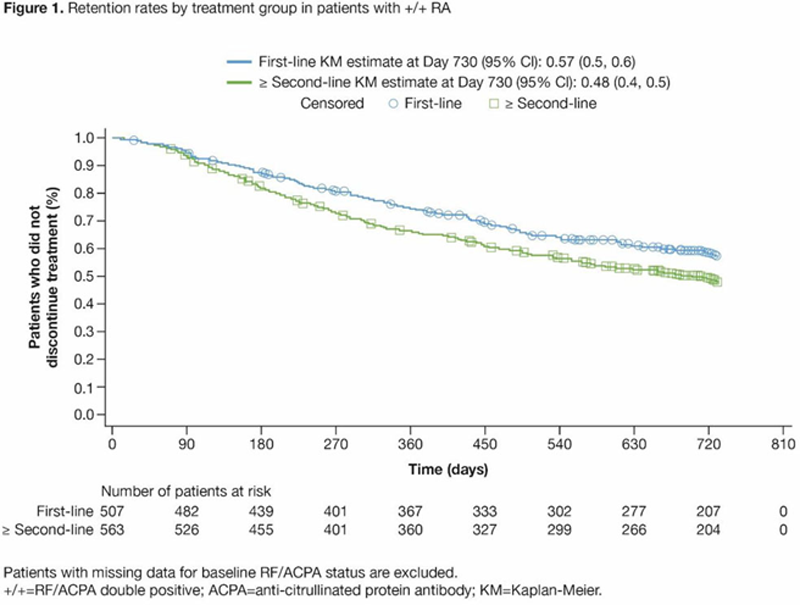
Conclusion: In this real-world analysis, patients with +/+ RA treated with first-line abatacept had higher retention than patients receiving abatacept as a ≥ second-line therapy. Remission rates on abatacept were higher in patients with +/+ RA versus –/– RA. These results support early treatment with abatacept and highlight the importance of further evaluating precision medicine approaches in RA.
REFERENCES:
[1]Smolen JS, et al. Ann Rheum Dis 2020;79:685–699.
[2]Alten R, et al. Ann Rheum Dis 2019;78(suppl 2):A1639.
Acknowledgements: Professional medical writing and editorial assistance was provided by Lindsay Craik at Caudex and was funded by Bristol Myers Squibb. This study was funded by Bristol Myers Squibb.
Disclosure of Interests: Rieke Alten Speakers bureau: AbbVie, Bristol Myers Squibb, Gilead, Janssen, Lilly, Pfizer, Consultant of: AbbVie, Bristol Myers Squibb, Gilead, Janssen, Lilly, Pfizer, Grant/research support from: AbbVie, Bristol Myers Squibb, Gilead, Janssen, Lilly, Pfizer, Xavier Mariette Consultant of: Bristol Myers Squibb, Galapagos, Gilead, GlaxoSmithKline, Janssen, Pfizer, UCB, Rene-Marc Flipo Speakers bureau: AbbVie, Bristol Myers Squibb, Janssen, Lilly, Medac, Merck Sharp & Dohme, Novartis, Pfizer, Roche-Chugai, Grant/research support from: Amgen, Janssen, Novartis, Pfizer, Roberto Caporali Speakers bureau: AbbVie, Amgen, Bristol Myers Squibb, Celltrion, Fresenius Kabi, Galapagos, Gilead, Lilly, Merck Sharp & Dohme, Pfizer, Roche, Samsung Bioepis, Sanofi, UCB, Consultant of: Galapagos, Gilead, Janssen, Lilly, Merck Sharp & Dohme, Maya H Buch Speakers bureau: AbbVie, Consultant of: AbbVie, Eli Lilly, Gilead, Merck Serono, Pfizer, Roche, Sanofi, Grant/research support from: Gilead, Pfizer, Roche, UCB, Yusuf Patel: None declared, Raimón Sanmartí Speakers bureau: AbbVie, Bristol Myers Squibb, Gebro, Janssen, Lilly, Merck Sharp & Dohme, Pfizer, Roche, Sanofi, Consultant of: AbbVie, Bristol Myers Squibb, Gebro, Lilly, Merck Sharp & Dohme, Pfizer, Roche, Sanofi, Grant/research support from: Bristol Myers Squibb, Merck Sharp & Dohme, Pfizer, Sara Marsal Speakers bureau: Bristol Myers Squibb, Celgene, Pfizer, Roche, Sanofi, UCB, Consultant of: AbbVie, Bristol Myers Squibb, Celgene, Galapagos, Merck Sharp & Dohme, Pfizer, Roche, Sanofi, UCB, Grant/research support from: AbbVie, Bristol Myers Squibb, Celgene, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, Roche, Sanofi, UCB, M.T. Nurmohamed Speakers bureau: AbbVie, Bristol Myers Squibb, Eli Lilly, Roche, Sanofi, Consultant of: AbbVie, Celgene, Celltrion, Eli Lilly, Janssen, Grant/research support from: AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Janssen, Merck Sharp & Dohme, Mundipharma, Novartis, Pfizer, Roche, Sanofi, Hedley Griffiths Consultant of: AbbVie, Gilead, Janssen, Novartis, Peter Peichl: None declared, Bettina Bannert: None declared, Adrian Forster: None declared, Melanie Chartier Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Sean Connolly Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Yedid Elbez Consultant of: Bristol Myers Squibb, Christiane Rauch Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Vadim Khaychuk Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Karissa Lozenski Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb