fetching data ... 
Background: Recommendations for the management of patients with RA who achieve stable clinical remission ≥6 months with conventional synthetic (cs) disease-modifying anti-rheumatic drugs (DMARDs) are to taper (with the aim of potentially stopping), although there are currently no validated biomarkers permitting prediction of sustained remission.
Objectives: To assess the rate of sustained remission over 12 months In RA patients in remission, who received either (i) structured tapering of csDMARDs or (ii) continuation of current therapy, focusing on the value of imaging and immunological biomarkers as well as patient-reported outcome measures (PROs).
Methods: RA patients (n=200) prospectively attending a remission clinic, fulfilling DAS28(3v)CRP<2.6 for ≥6 months on stable csDMARD therapy (mono or combination therapy & no corticosteroids) were included. Patients were offered the choice of structured cs-DMARD tapering according to a pre-defined protocol (
csDMARD tapering schedule
| Drug | Baseline Dose | Taper 1 | Taper 2 | Taper 3 | Taper 4 | Taper 5 |
| Hydroxychloroquine | 200mg bd | 200mg od | Stop | - | - | - |
| Hydroxychloroquine | 200mg od | Stop | - | - | - | - |
| Sulfasalazine | 1.5g bd | 1g bd | 1.5g od | 500mg bd | 500mg od | Stop |
| Sulfasalazine | 1g bd | 1.5g od | 500mg bd | 500mg od | Stop | - |
| Sulfasalazine | 500mg bd | 500mg od | Stop | - | - | - |
| Sulfasalazine | 500mg od | Stop | - | - | - | - |
| Methotrexate | 25mg/week | 15mg/week | 7.5mg/week | No change | Stop | - |
| Methotrexate | 15mg/week | 7.5mg/week | No change | Stop | - | - |
| Methotrexate | 7.5mg/week | No change | Stop | - | - | - |
NB: Patients were seen 3-monthly. If they remained in remission following tapering, they proceeded to the next taper unless there is a significant clinical reason not to taper at the time of assessment (as per standard care). Order of cs-DMARD tapering applies to patients on dual/triple therapy. All but 5 (112) were on methotrexate.
Results: The decision to taper treatment was associated with male gender, longer remission duration, normal CRP and lower grey scale scores (p<0.05). Of those who tapered 64% (75/117) remained in clinical remission at 12 months, compared to 80% (66/83, p=0.018) of patients who remained on stable treatment. At 15 months 11/117 (10%) had successfully stopped therapy.
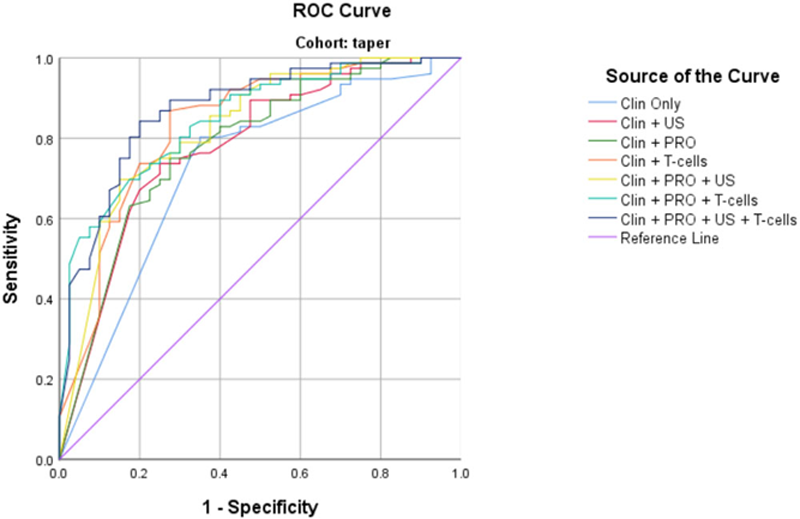
In the tapering group, higher CRP, TJC and IRC were consistently associated with inability to sustain remission, as well as higher scores for several PROs (p<0.05) with a trend for total PD (P=0.066). Predicting sustained remission was modelled and retained RAQoL, total PD and a T-cell subset (
AUROC Analysis of tapering cohort data
In the non-tapering group, higher CRP/ESR, SJC and shorter disease duration (p<0.05) were associated with flare. No parameter was able to predict sustained remission.
Conclusion: In patients who chose to taper, the combination of clinical, PRO, US and T-cell parameters demonstrated added value for predicting sustained remission (85% accuracy) compared to clinical parameters alone. Different biomarkers were associated with sustained remission on continued therapy. These data may assist with informed tapering of csDMARDs.
Disclosure of Interests: None declared