fetching data ... 
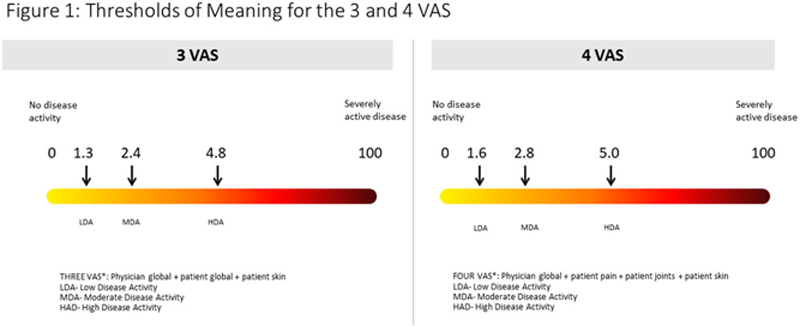
Background: There is a recognised need for a continuous composite measure of disease activity for the assessment of Psoriatic Arthritis (PsA) in routine clinical settings to allow objective assessment of response and implementation of treat to target. 1 Longer multidimensional measures are considered less feasible in routine care and a number of shorter measures have been proposed including, the Disease Activity Score for Psoriatic Arthritis (DAPSA), Disease Activity Score 28 (DAS28), the 3 Visual Analogue Scale (VAS) (comprising physician global VAS, patient global VAS and patient skin VAS) or 4 VAS (comprising physician global VAS, patient pain VAS, joint VAS and patient skin VAS). Testing of these measures in clinical trial datasets has been suggested but thresholds of meaning have not been established. 2
Objectives: To estimate clinically relevant thresholds of disease activity and improvement for composite measures for routine clinical practice in PsA.
Methods: Clinical and patient reported outcome measures were assessed in patients fulfilling CASPAR criteria for PsA at three consecutive follow up visits in a UK multicentre observational study. Participants underwent clinical assessment and completed patient reported measures including health anchor questions. Estimates for Minimal Detectible Change (MDC) were derived using 1.96*2*Standard Error of the Mean (SEM). Minimal Clinically Important Difference (MCID) for improvement were derived using the health anchor method and two distribution methods (
Minimal Clinically Important Difference (MCID) and Minimal detectable change (MDC)
| ANCHOR (MEDIAN) | DISTRIBUTION#1 | DISTRIBUTION #2 | MDC | |
| CPDAI | 0.5 | 1.49 | 1.5 | 4.16 |
| GRACE | 0.26 | 0.6 | 0.77 | 2.18 |
| PASDAS | 1.22 | 0.64 | 0.76 | 1.58 |
| DAS28 | 0.2 | 0.85 | 0.62 | 1.46 |
| 3VAS | 1.13 | 1.16 | 0.91 | 3.12 |
| 4VAS | 1.11 | 0.96 | 0.94 | 2.45 |
| DAPSA | 7.25 | 9.09 | 10.40 | 35.63 |
Disease Activity Score for Psoriatic Arthritis (DAPSA); Psoriatic Arthritis Disease Activity Score (PASDAS); Composite Psoriatic Arthritis Disease Activity Index (CPDAI); Disease Activity Score 28 (DAS28).
Distribution #1: Baseline standard deviation (sd) * √ 1 – Cronbach’s alpha
Distribution #2: 0.5 * baseline sd
Minimal detectable change (MDC): 1.96*2*SEM where SEM = baseline sd √1 - ICC
Results: 139 subjects were recruited (59 male, 80 female, mean (range) age (years) 52.7 (19 – 83), mean (range) duration of psoriasis (years) 21.9 (2 – 71), mean (range) duration of psoriatic arthritis (years) 6.1 (0 – 41). Cut-off values for low, moderate and high disease activity were 1.3, 2.4, and 4.8 for the 3 Vas and 1.6, 2.8 and 5.0 for the 4 VAS (
Conclusion: We report estimates of clinically relevant improvements for continuous composite measures in PsA and estimates of low, moderate and high disease activity for the 3 and 4 VAS scales. The thresholds of meaning can now be tested in independent observational and clinical trial datasets.
REFERENCES:
[1]Coates et al 2018 A&R Mar;70(3):345-355.
[2]Tillett W et al 2021 J Rheum In Press
Acknowledgements Funding: This report is independent research funded by the National Institute for Health Research, Programme Grants for Applied Research [Early detection to improve outcome in patients with undiagnosed PsA (‘PROMPT’), RP-PG-1212-20007]. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Disclosure of Interests: William Tillett Speakers bureau: AbbVie, Amgen, Celgene, Lilly, Janssen, Novartis, MSD, Pfizer, and UCB, Consultant of: AbbVie, BMS, Celgene, Lilly, Janssen, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, BMS, Janssen, Novartis, Pfizer, and UCB., Julia Day: None declared, Neil McHugh: None declared, Oliver FitzGerald Speakers bureau: AbbVie, BMS, Celgene, Lilly, Janssen, Novartis, Pfizer, and UCB, Consultant of: AbbVie, BMS, Celgene, Lilly, Janssen, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, BMS, Janssen, Novartis, Pfizer, and UCB., Laura C Coates Speakers bureau: AbbVie, Amgen, Biogen, Celgene, Gilead, Eli Lilly, Janssen, Medac, Novartis, Pfizer, and UCB., Consultant of: AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, Janssen, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Amgen, Celgene, Eli Lilly, Pfizer, and Novartis, Philip Helliwell: None declared