fetching data ... 
Background: Enthesitis is a key musculoskeletal manifestation of psoriatic arthritis (PsA). EULAR guidelines recommend biologics for patients with enthesitis and an inadequate response to or intolerance of nonsteroidal anti-inflammatory drugs, although no guidance on specific biologics is offered. In the EXCEED head-to-head, double-blind study (NCT02745080), secukinumab (SEC) and adalimumab (ADA) showed a similar efficacy in joints and in resolution of enthesitis at Week 52 for patients with PsA, 1 although a detailed analysis of enthesitis was not conducted.
Objectives: To explore detailed enthesitis treatment response, including temporal and additional enthesitis assessment data, in patients with PsA treated with SEC or ADA over 52 weeks.
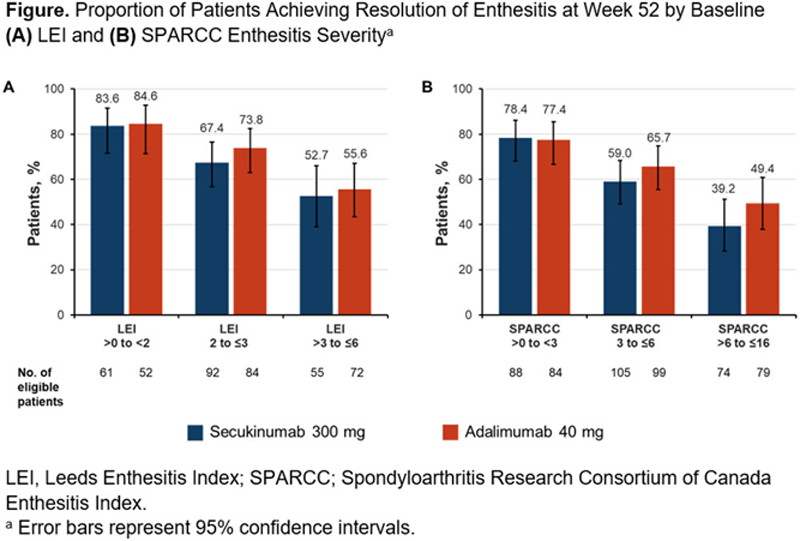
Methods: In this post hoc analysis, patient data from EXCEED were grouped by presence or absence of baseline enthesitis based on the Leeds Enthesitis Index (LEI) and the Spondyloarthritis Research Consortium of Canada Enthesitis Index (SPARCC). Baseline characteristics of these groups were summarized. Median time to resolution of LEI/SPARCC enthesitis score in patients receiving SEC or ADA was assessed using Kaplan-Meier analysis. Efficacy was further assessed among the enthesitis subset by LEI and SPARCC change from baseline, resolution of enthesitis (LEI/SPARCC) at Weeks 24 and 52, and resolution of enthesitis at Week 52 by baseline enthesitis severity. Relapse of enthesitis after a first resolution was evaluated at Weeks 24 and 52. Missing data were imputed by nonresponder imputation.
Results: Baseline demographics were well balanced in the LEI/SPARCC enthesitis subsets, although a higher proportion of all patients with enthesitis were women vs those with no enthesitis (LEI: 54.6% vs 40.5%; SPARCC: 53.2% vs 36.2%). Patients with baseline enthesitis had higher disease activity vs patients without enthesitis (LEI/SPARCC enthesitis vs no LEI/SPARCC enthesitis: tender joint count of 78 joints [22.8/22.1 vs 15.8/13.8], Health Assessment Questionnaire-Disability Index [1.3/1.3 vs 1.1/1.1], and mean Psoriasis Area and Severity Index [6.4/6.1 vs 5.1/5.3]). Median time to resolution of LEI and SPARCC enthesitis was similar between patients receiving either SEC or ADA (
Conclusion: In EXCEED, patients with baseline enthesitis presented with higher disease burden, consistent with the FUTURE trials. 2 SEC and ADA showed similar kinetics of response and efficacy on enthesitis, irrespective of baseline enthesitis severity.
REFERENCES:
[1]McInnes IB, et al. Lancet . 2020;395(10235):1496-1505.
[2]Coates LC, et al. Arthritis Res Ther. 2019;21(1):266.
Clinical Improvements Among Patients With Baseline LEI or SPARCC Enthesitis Treated with Secukinumab or Adalimumab (nonresponder imputation)
|
Secukinumab
|
Adalimumab
|
|||
| Outcomes a |
LEI
|
SPARCC
|
LEI
|
SPARCC
|
| Baseline enthesitis count, mean (SD) | 2.6 (1.5) | 5.0 (3.8) | 2.8 (1.6) | 5.4 (4.0) |
| Median time to enthesitis resolution, days (95% CI) | 85 (57–113) | 113 (85–169) | 85 (57–86) | 88 (85–114) |
| Enthesitis count, mean improvement from baseline (SD) | ||||
| Week 24 | −1.6 (1.6) | −3.3 (3.5) | −1.6 (1.6) | −3.1 (3.5) |
| Week 52 | −1.8 (1.6) | −3.6 (3.2) | −2.1 (1.7) | −3.9 (3.8) |
| Resolution of enthesitis, n (%) | ||||
| Week 24 | 116 (49.6) | 138 (45.8) | 115 (43.6) | 144 (43.5) |
| Week 52 | 142 (60.7) | 160 (53.2) | 146 (55.3) | 170 (51.4) |
| Enthesitis relapse, n/M (%) | ||||
| Week 24 | 37/210 (17.6) | 38/274 (13.9) | 49/232 (21.1) | 47/293 (16.0) |
| Week 52 | 40/208 (19.2) | 56/267 (21.0) | 32/208 (15.4) | 41/263 (15.6) |
LEI, Leeds Enthesitis Index; M, number of evaluable patients; SPARCC; Spondyloarthritis Research Consortium of Canada Enthesitis Index.
a Based on respective enthesitis measures.
Acknowledgements: This study was funded by Novartis Pharma AG. The authors thank Richard Karpowicz, PhD, of Health Interactions, Inc, for providing medical writing support/editorial support, which was funded by Novartis Pharmaceuticals Corporation, East Hanover, NJ, in accordance with Good Publication Practice (GPP3) guidelines (
Disclosure of Interests: Gurjit S. Kaeley Consultant of: Novartis Pharmaceuticals Corporation, Georg Schett Speakers bureau: AbbVie, Bristol Myers Squibb, Celgene, Janssen, Eli Lilly, Novartis, and Pfizer, Consultant of: AbbVie, Bristol Myers Squibb, Celgene, Janssen, Eli Lilly, Novartis, and UCB, Grant/research support from: Bristol Myers Squibb, Celgene, GSK, Eli Lilly, and Novartis, Philip G Conaghan Consultant of: or Speakers bureau: AbbVie, AstraZeneca, Bristol Myers Squibb, Eli Lilly, EMD Serono, Flexion Therapeutics, Galapagos, Gilead, Novartis, and Pfizer, Grant/research support from: UK National Institute for Health Research (NIHR) Leeds Biomedical Research Centre, Dennis McGonagle Speakers bureau: Roche, Sobi, and Novartis, Grant/research support from: Novartis, Frank Behrens Consultant of: Pfizer, AbbVie, Sanofi, Lilly, Novartis, Genzyme, Boehringer, Janssen, Merck Sharp & Dohme, Celgene, Roche, and Chugai, Grant/research support from: Pfizer, Janssen, Chugai, Celgene, and Roche, and has received investigator fees from Eli Lilly, Philippe Goupille Grant/research support from: and/or Consultant of/Speakers bureau: AbbVie, Amgen, Biogen, Bristol Myers Squibb, Celgene, Chugai, Janssen, Lilly, Medac, Merck Sharp & Dohme, Nordic Pharma, Novartis, Pfizer, Sanofi, and UCB, Corine Gaillez Employee of: Novartis Pharma AG, Bhumik Parikh Employee of: Novartis Pharmaceuticals Corporation, Xiangyi Meng Employee of: Novartis Pharmaceuticals Corporation, Catherine Bakewell Consultant of: and/or Speakers bureau: AbbVie, Novartis, Pfizer, Janssen, UCB, and Sanofi Genzyme/Regeneron