fetching data ... 
Background: Sick leave (SL) represents an often poorly studied adverse work outcome especially in early axSpA, with speculation around the potential role of clinical and socioeconomic (SE) factors.
Objectives: To investigate the occurrence of SL and the impact of clinical and SE factors on SL in early axSpA.
Methods: Patients with a clinical diagnosis of axSpA from the DESIR cohort up to 5 years of follow-up (6-month visits in the first 2 years, followed by annual visits) were studied. Time to SL and potential baseline and time-varying predictors were explored, with a focus on SE variables: age, gender, smoking status since last visit, ethnicity (Caucasian vs other), job type based on ‘collar’ (blue vs white), educational status (low vs high -university), marital status (married vs not) and parental status (number of children); and clinical factors including disease activity (ASDAS/BASDAI), function (BASFI), mobility (BASMI), at each time point. The incidence of SL was calculated as the number of SL events over the total number of person-days under observation. Univariable analyses, followed by collinearity and interaction tests, guided subsequent multivariable Cox survival model building.
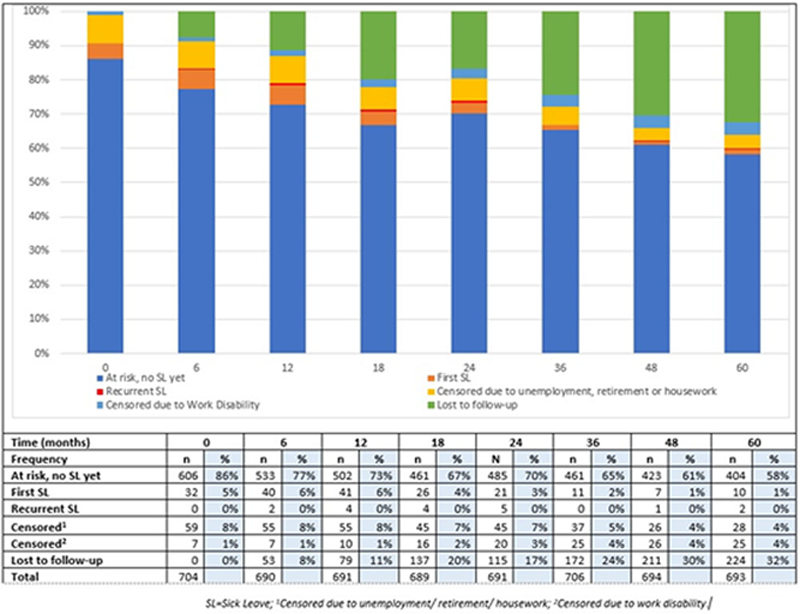
Results: In total, 704 axSpA patients with work-related data were included in this study: mean (SD) age 33.8 (8.6); 46% male. At baseline, 80% of patients were employed; of these, 5.7% reported being on SL, with people shifting in and out of different work states over time. The distribution of first and recurrent SL episodes over time is shown in the
Univariable and multivariable model analyses with Sick Leave as outcome.
| Type of analysis | Univariable analysis | Multivariable model |
| HR (95% CI) | HR (95% CI)
|
|
| Explanatory variables | ||
| Age | 1.04 (1.01, 1.08) | 1.05 (1.01, 1.09) |
| Male gender | 0.37 (0.19, 0.74) | 0.41 (0.20, 0.86) |
| High education | 0.33 (0.17, 0.61) | 0.48 (0.24, 0.95) |
| Marital status | 2.44 (1.12, 5.27) | NS |
| ASDAS (CRP) | 1.83 (1.34, 2.50) | 1.49 (1.04, 2.13) |
| BASFI, 0-10 | 1.24 (1.09, 1.40) | * |
| BASMI, 0-10 | 1.76 (1.31, 2.38) | * |
| Comorbidity count | 1.77 (1.22, 2.57) | NS |
| HLA-B27 positive | 0.51 (0.28, 0.93) | NS |
| Smoking (current vs not) | 2.40 (1.31, 4.37) | 2.55 (1.32, 4.91) |
| NSAID score last week, 0-400 | 1.01 (1.00, 1.01) | NS |
| Oral Corticosteroid use (vs no) | 3.90 (1.80, 8.46) | NS |
| TNF use | 2.86 (1.55, 5.28) | 2.41 (1.27, 4.58) |
*Variables tested in models separate from ASDAS. NS=Not significant in multivariable model.
Distribution of first and recurrent sick leave episodes over time in the study population at risk.
Conclusion: In this early axSpA cohort of young, working-age individuals, older age and worse disease activity were associated with more SL, whereas male gender and higher education were associated with less SL. The findings suggest a role of SE factors such as gender and level of education in adverse work outcomes, alongside active disease.
Disclosure of Interests: None declared