fetching data ... 
Background: EULAR recommends doppler ultrasound (US) as the first line imaging in patients with Giant Cell Arteritis (GCA) suspect. Traditionally, US non-compressive halo sign has been used for diagnosis but prospective studies on response and disease monitoring are lacking
Objectives: The HAS GCA study has the objective of prospectively assessing role of US in diagnosis, prognosis and monitoring in newly diagnosed GCA. We report early baseline and up to month 3 data on our current recruitment in a study that has suffered disruption from the pandemic
Methods: HAS GCA (IRAS#264294) is an ongoing, prospective, multicentre study recruiting from referrals of suspected GCA to fast track clinics. The objective is to recruit 270 patients, including 68 GCA patients. Based on the Southend GCA clinical pre-test probability score (SPTPS) 1 , patients were stratified in to low, intermediate and high risk categories 2 . Temporal and axillary US Halo Scores were calculated from the halo thickness and extent in bilateral temporal arteries, parietal and frontal branches and axillary arteries. These individual scores were summed (TA Halo Score x1 plus; AA Halo Score x3) to generate a Total Halo Score (THS) 3 .
Mann Whitney U test and Fisher’s exact test were used to compare baseline features between GCA and controls. Wilcoxon signed rank test was used to evaluate disease features at baseline and at 3 months in GCA patients. Sensitivity (Sn) and Specificity (Sp) were calculated, where applicable. P value <0.05 is statistically significant
Results: Ninety-three patients (29 GCA, 64 controls) have been recruited thus far: 18 completed 3-month follow up assessment; 4 were lost to follow up (2 died, 2 withdrew consent due to pandemic). Demographics, clinical features, and US results are shown (
Baseline features of GCA patients and controls.
| GCA (n=29) | Controls (n=64) | P-value | |
| Age, median (IQR) | 75 (71-80) | 67 (61.25 – 75.0) | 0.001 |
| Female, n (%) | 15 (42) | 50 (78) | 0.01 |
| SPTPS category, n (%) | |||
| Low risk | 0 (0) | 31 (48) | <0.001 |
| Intermediate risk | 7 (24) | 25 (39) | 0.24 |
| High risk | 22 (76) | 8 (13) | <0.001 |
| Halo score (HS), median (range) | |||
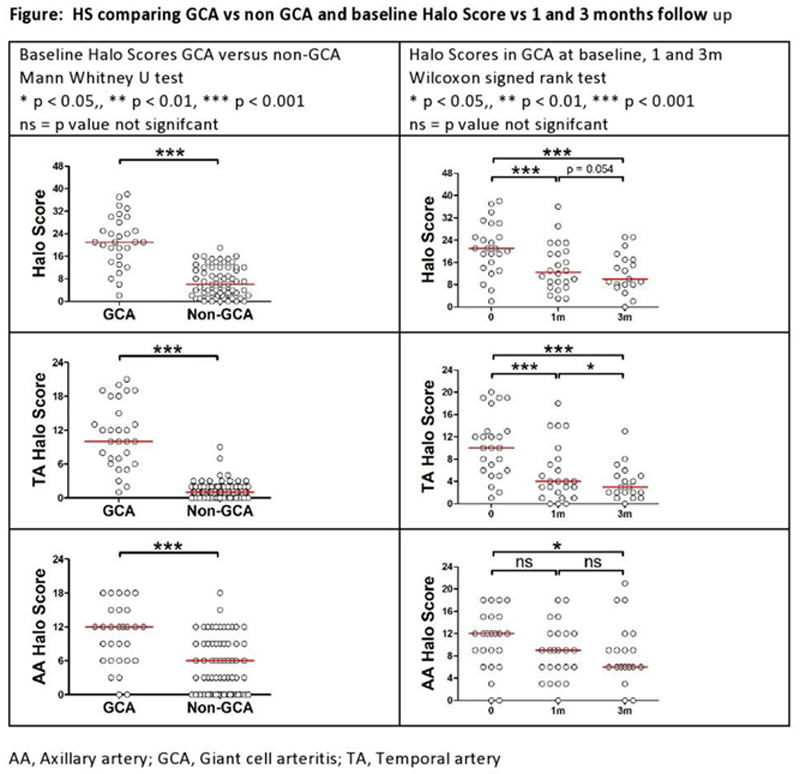
| Temporal artery HS | 10 (1-21) | 1 (0-9) | <0.001 |
| Axillary artery HS | 12 (0-18) | 6 (0-18) | <0.001 |
| Total HS | 21 (2-38) | 6 (0-19) | <0.001 |
| Clinical features, n (%) | |||
| Temporal headache | 21 (72) | 40 (63) | 0.48 |
| Scalp tenderness | 17 (59) | 31 (48) | 0.38 |
| Jaw claudication | 19 (66) | 4 (6) | <0.001 |
| PMR symptoms | 16 (55) | 6 (9) | <0.001 |
| Constitutional symptoms | 17 (59) | 18 (28) | 0.006 |
| Visual disturbance | 18 (62) | 38 (59) | 1 |
| Vision loss | 7 (24) | 4 (6) | 0.03 |
Among GCA patients, 23 had cranial, 2 large-vessel and 4 mixed phenotypes (cranial plus large vessel) disease.
Jaw claudication (66%) and polymyalgic symptoms (55%) were the dominant features in GCA patients. Median age 75 years in GCA (42% females) and 67 years in controls (78% females). GCA and controls were stratified by SPTPS to Low risk (0% vs 48%; Sn-undefined, Sp-97), Intermediate risk (24% vs 39%; Sn-100, Sp-100) and High risk (76% vs 13%; Sn-95, Sp-88). Optimal SPTPS cut-off point was ≥12 (Sn-93, Sp-86); ≥10 (Sn-100 & Sp-69).
Median THS was 21 in GCA and 6 in controls. Optimal cut-off Halo Score in diagnosis was TAHS ≥5 (Sn-90, Sp-98), AAHS ≥11 (Sn-55, Sp-80), THS ≥18 (Sn-72%, Sp-98%). Among the 18 patients who completed 3-months follow up, median TAHS, AAHS and THS reduced from 10 to 2.5, 12 to 6 and 21 to 10, respectively (
Conclusion: Along with SPTPS, Halo Score successfully discriminates GCA from non GCA mimics. HS is effective in showing 3-month response and may be a useful marker to monitor GCA disease activity.
REFERENCES:
[1]Laskou F et al. A probability score to aid the diagnosis of suspected giant cell arteritis. Clin Exp Rheumatol. 2019
[2]Sebastian A et al. Probability-based algorithm using ultrasound and additional tests for suspected GCA in a fast-track clinic. RMD Open. 2020
[3]Sebastian A et al. Halo score (temporal artery, its branches and axillary artery) as a diagnostic, prognostic and disease monitoring tool for Giant Cell Arteritis (GCA). BMC Rheumatol. 2020
Disclosure of Interests: Alwin Sebastian: None declared, Alessandro Tomelleri: None declared, Abdul Kayani: None declared, Mohammad Tariq: None declared, Diana Prieto-Peña: None declared, Sue Inness: None declared, Jo Jackson: None declared, Kornelis van der Geest Speakers bureau: Roche, Bhaskar Dasgupta Speakers bureau: Roche, GSK, BMS, Sanofi, Abbie, Grant/research support from: Roche