fetching data ... 
Background: Sustained remission is the ultimate goal in the management of rheumatoid arthritis (RA) but is infrequently achieved. After conventional therapy, TNFi (tumour necrosis factor inhibitor) has a strong track record for achieving remission. Existing studies suggest variable effect of RA and TNFi on various cellular components of the full blood count (FBC), but their relationship with loss of remission (LOR) is unclear.
Objectives: To investigate whether cellular changes in the FBC can predict LOR (remission defined as DAS28-ESR≤2.6) in patients with RA receiving TNFi, adjusted using key clinical factors.
Methods: Real-world clinical and routine laboratory data were analysed from two independent cohorts of adult RA patients, who were started on their first TNFi (from 2009 to December 2019), and went into remission. Data was extracted in October 2020. A linear mixed model was used to investigate longitudinal changes of different components of FBC and CRP, stratified by LOR, and grouped by years of follow-up. Pairwise post-hoc comparisons were performed by Bonferroni correction. Area Under the Receiver Operating Characteristics (AUROC) of cellular changes in FBC components to predict LOR at different time points were calculated. Latent class mixed models were used to investigate trajectories of change in cellular components of the FBC from baseline to one year. Further survival analysis to predict LOR of TNFi was done by using the latent class model and adjusted by clinical parameters, demographics and concomitant treatment.
Results: 92 and 43 biologic-naïve RA patients who attained remission were included from cohorts 1 and 2 respectively. 73 (54%) were treated with adalimumab and 62 (46%) with etanercept. 87 (64%) of patients lost remission over a 10-year period with median time to LOR of 3.3 years (95% CI 2.6-3.7).
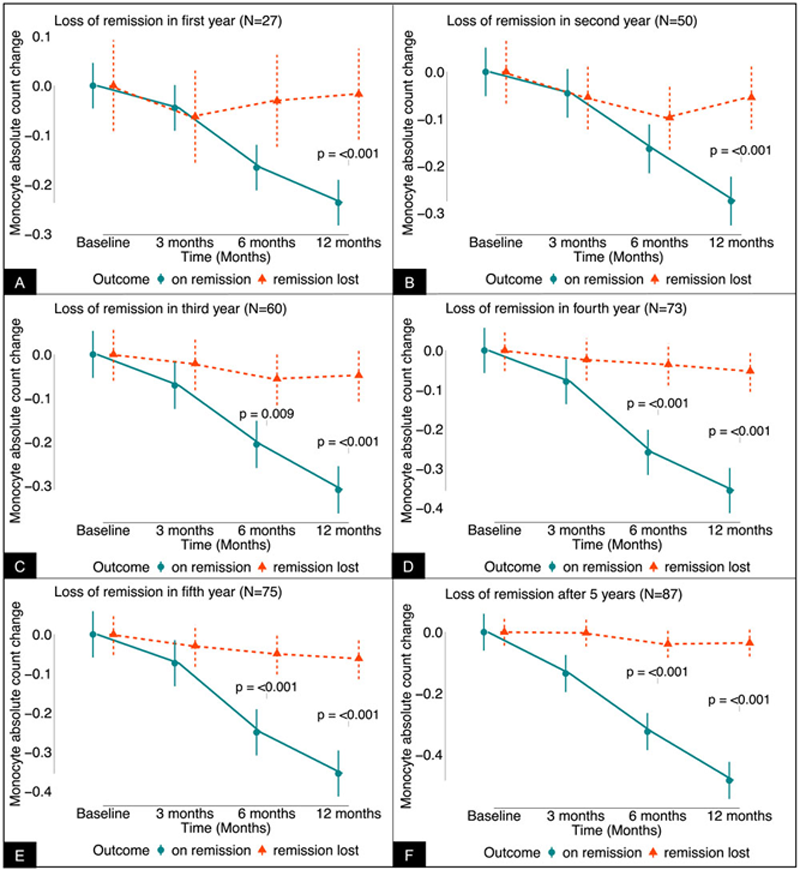
Among the cellular components of FBC, monocyte count changes in the first year after initiation of TNFi fell significantly in those who maintained remission over the five years of follow-up, compared to those who lost remission [p<0.001 for all years evaluated] (
Conclusion: In seropositive RA patients treated with TNFi, a reduction of total monocyte count in the first year was associated with maintenance of remission in subsequent years. Further studies are required to determine whether these effects are specific to TNFi or reflect sustained remission in RA irrespective of therapy.
(A-F). Mean change (with 95% confidence interval) in absolute count of monocyte after initiation of tumour necrosis factor inhibitor grouped by years of follow-up and stratified by loss of remission. N = number indicate cumulative number of patients who lost remission by the end of each year.
Acknowledgements: Muhammad Shipa is funded by Versus Arthritis. Su-Ann Yeoh is funded by the Royal College of Physicians, Rosetrees Trust, NIHR University College London Hospitals Biomedical Research Centre, UCLH Charities, and Versus Arthritis. Michael Ehrenstein is supported (in part) by the University College London Hospital Biomedical Research Centre. None of the funding bodies have been involved in preparation of this manuscript.
Disclosure of Interests: None declared