fetching data ... 
Background: The efficacy and safety of baricitinib (BARI), an oral selective Janus kinase (JAK)1/JAK2 inhibitor, were evaluated in the randomized, controlled trial, RA-BEAM (NCT01710358), in patients (pts) with active rheumatoid arthritis (RA) and inadequate responses (IR) to methotrexate (MTX). 1,2,3
Objectives: To compare the time to onset and magnitude of improvement across different patient-reported outcomes (PROs) of BARI, adalimumab (ADA) and placebo (PBO) during the first 12 weeks of treatment in RA-BEAM.
Methods: 1,305 patients on stable background MTX were randomized 3:3:2 to PBO, BARI 4 mg, or ADA 40 mg. In this intent-to-treat analysis, least-squares mean changes and percentage changes from baseline were assessed up to Week 12 for pain (0-100 mm visual analog scale [VAS]), SF-36 physical component summary (PCS, 0-100), morning joint stiffness (MJS) severity (0-10), Health Assessment Questionnaire-Disability Index (HAQ-DI, 0-3), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F, 0-52), and Patient Global Assessment of disease activity (PtGA, 0-100 mm VAS) scores. PROs were compared between treatments with ANCOVA; the model included change from baseline as the response variable, baseline of interest, regional baseline, joint erosion status, and treatment as explanatory variables. Last-observation-carried-forward was applied to impute missing data. Speed of onset and magnitude of PRO improvement are presented in spydergrams.
Results: Statistically significant improvements (P<0.05) with BARI and ADA vs. PBO were reported as early as Week 1 for pain, MJS severity, HAQ-DI, and PtGA and at Week 4 for FACIT-F and SF-36 PCS scores. Statistically significantly larger improvements (P<0.05) with BARI vs. ADA were observed as early as Week 2 for pain, PtGA, Week 3 for MJS severity, and Week 4 for HAQ-DI and SF-36 PCS scores. These improvements were maintained to Week 12.
Conclusion: Among MTX-IR pts, BARI and ADA treatment resulted in improvements across all PROs by Week 4, and as early as Week 1, for all but FACIT-F and SF-36 PCS scores. Statistically significant larger improvements for BARI compared with ADA were reported for all PROs, except FACIT-F, by Week 12.
REFERENCES:
[1]Taylor et al. NEJM, 2017;376: 652-62
[2]Keystone et al. Ann Rheum Dis, 2017;76:1853-61
[3]Strand et al. Ann Rheum Dis, 2020; 79: 599-600
Change from baseline in patient-reported outcomes at Weeks 4 and 12
| Week 4 | Week 12 | |||||
| LSM Change from Baseline | PBO | ADA | BARI | PBO | ADA | BARI |
| Pain VAS | -12.6 | -22.3*** | -27.1***†† | -17.1 | -26.4*** | -31.5***†† |
| SF-36 PCS | 3.0 | 5.7*** | 6.9***†† | 4.2 | 7.2*** | 8.7***†† |
| MJS severity | -0.9 | -1.5*** | -1.9***†† | -1.4 | -2.0*** | -2.5***††† |
| HAQ-DI | -0.26 | -0.47*** | -0.54***† | -0.34 | -0.56*** | -0.66***†† |
| FACIT-F | 5.2 | 6.9** | 7.8*** | 6.7 | 8.7*** | 9.1*** |
| PtGA | -14.2 | -23.7*** | -26.8***† | -16.7 | -26.6*** | -31.2***†† |
*p≤0.05, **p≤0.01, ***p≤0.001 vs PBO; †p≤0.05, ††p≤0.01, †††p≤0.001 vs. ADA
ADA: adalimumab; BARI: baricitinib; FACIT-F: Functional Assessment of Chronic Illness Therapy-Fatigue; HAQ-DI: Health Assessment Questionnaire-Disability Index; MJS: morning joint stiffness; PBO: placebo; PCS: physical component scale; PtGA: Patient Global Assessment; VAS: visual analog scale
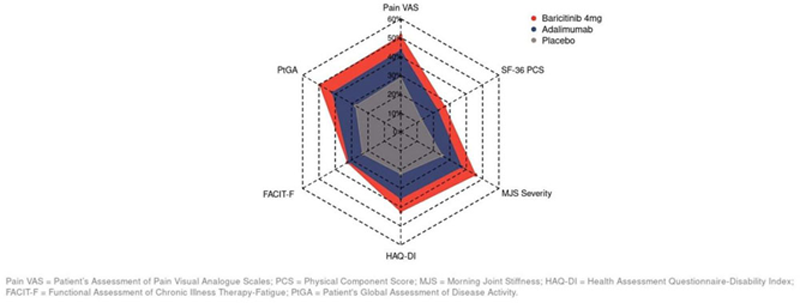
Percentage improvement from baseline to Week 12 in PROs of patients with RA in RA-BEAM
Acknowledgements: The authors would like to acknowledge Molly Tomlin, with Eli Lilly and Company, for medical writing and project management support
Disclosure of Interests: Vibeke Strand Consultant of: AbbVie, Amgen, Arena, AstraZeneca, Bayer Pharmaceuticals, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Eli Lilly and Company, Galapagos NV, Genentech, Gilead, GlaxoSmithKline, Ichnos, Inmedix, Janssen, Kiniksa, Merck, Myriad Genetics, Novartis, Pfizer, Regeneron, Samsung, Sandoz, Sanofi, Scipher, Setpoint, Sun Pharma, and UCB Pharma, Anthony Sebba Speakers bureau: Eli Lilly and Company, Genentech, Sanofi, Regeneron, Consultant of: Amgen, Eli Lilly and Company, Genentech, Gilead Sciences, Novartis, Sanofi, Regeneron, Bochao Jia Shareholder of: Eli Lilly and Company, Employee of: Eli Lilly and Company, Julie Birt Shareholder of: Eli Lilly and Company, Employee of: Eli Lilly and Company, Amanda Quebe Shareholder of: Eli Lilly and Company, Employee of: Eli Lilly and Company, Hong Zhang Consultant of: Eli Lilly and Company, Peter C. Taylor Consultant of: AbbVie, Biogen, Galapagos, Gilead, GlaxoSmithKline, Janssen, Lilly, BMS, Pfizer, Roche, Celltrion, Sanofi, Nordic Pharma, Fresenius and UCB, Grant/research support from: Celgene, Galapagos, Janssen, Lilly