fetching data ... 
Background: The Janus kinase-1 preferential inhibitor filgotinib (FIL) improved signs and symptoms of rheumatoid arthritis (RA) in the FIL clinical program. 1–3
Objectives: To assess FIL safety across regions.
Methods: This was an analysis of patients (pts) meeting 2010 ACR/EULAR RA criteria in pooled phase (P)2 DARWIN 1–2 (D1–2), P3 FINCH 1–3 (F1–3), and long-term extension studies (DARWIN 3, FINCH 4). Data were analyzed by region: North America, South and Central America, Western Europe, Eastern Europe, Asia, South East (SE) Asia, and Other. Week (W)12 placebo (PBO)-controlled analysis included data from pts receiving once-daily FIL 100 mg (FIL100), FIL 200 mg (FIL200), or PBO for ≤12W (D1–2, F1–2); long-term as-treated data included pts from all 7 studies receiving FIL100 or FIL200; data after rerandomization were included and contributed to treatment received. Data presented as exposure-adjusted incidence rates (EAIRs)/100 patient-years of exposure (PYE) of treatment-emergent (TE) adverse events (TEAEs).
Results:
EAIR of TEAEs (placebo-controlled)
|
North America
|
South and Central America
|
Western Europe
|
Eastern Europe
|
Asia
|
South East Asia
|
Other
|
|
| TEAE | |||||||
| FIL200 a | 216.9 (162.5, 289.5) | 205.6 (155.1, 272.6) | 285.0 (188.6, 430.8) | 150.3 (119.3, 189.4) | 248.9 (180.6, 343.1) | 165.1 (104.0, 262.1) | 298.4 (150.3, 592.5) |
| FIL100 b | 182.2 (136.8, 242.7) | 159.2 (117.3, 216.1) | 285.7 (183.7, 444.3) | 146.4 (115.9, 185.0) | 246.9 (180.3, 338.1) | 153.7 (94.2, 251.0) | 263.5 (113.9, 609.2) |
| PBO C | 174.5 (130.3, 233.7) | 162.1 (118.8, 221.2) | 314.9 (200.7, 493.9) | 148.4 (117.6, 187.4) | 259.0 (188.0, 356.8) | 81.6 (40.8, 163.3) | 306.0 (142.8, 655.7) |
| TE serious AE | |||||||
| FIL200 a | 14.3 (6.0, 34.4) | 11.4 (3.7, 35.5) | 8.3 (1.2, 59.0) | 12.2 (5.2, 28.7) | 5.5 (0.8, 38.9) | 0.0 (0.0, ∞) | 49.6 (10.2, 144.9) |
| FIL100 b | 10.6 (4.0, 28.3) | 7.2 (1.8, 28.7) | 19.9 (5.0, 79.7) | 15.1 (6.8, 33.7) | 16.2 (5.2, 50.2) | 28.8 (9.3, 89.4) | 20.5 (0.5, 114.0) |
| PBO C | 16.1 (7.2, 35.9) | 7.5 (1.9, 30.0) | 29.6 (9.5, 91.7) | 4.6 (1.3, 15.8) | 11.4 (2.8, 45.5) | 10.2 (1.4, 72.4) | 0.0 (0.0, 69.2) |
| TEAE leading to discontinuation | |||||||
| FIL200 a | 8.6 (2.8, 26.6) | 3.8 (0.1, 21.2) | 16.6 (4.2, 66.5) | 12.9 (5.5, 30.5) | 0.0 (0.0, 20.2) | 9.2 (1.3, 65.1) | 16.5 (0.4, 92.1) |
| FIL100 b | 10.6 (4.0, 28.3) | 7.2 (0.9, 26.0) | 19.9 (5.0, 79.7) | 1.9 (0.2, 13.8) | 5.4 (0.1, 30.1) | 9.6 (1.4, 68.2) | 0.0 (0.0, 75.5) |
| PBO C | 5.4 (1.3, 21.5) | 0.0 (0.0, 13.8) | 9.9 (1.4, 70.0) | 12.9 (5.4, 30.7) | 17.1 (3.5, 49.9) | 20.4 (5.1, 81.6) | 0.0 (0.0, 69.2) |
Data presented as EAIR (95% CI)/100 patient-years
a N = 777, 179.8 PYE b N = 788, 181.6 PYE c N = 781, 178.4 PYE
A subject may contribute to more than one treatment group if they received more than one treatment of interest.
EAIR and corresponding 95% CI were estimated using Poisson regression model by treatment, including study and treatment with an offset of natural log of exposure time, except when 0 events occurred; Poisson model was not adjusted by study.
AE, adverse event; CI, confidence interval; EAIR, exposure-adjusted incidence rate; FIL, filgotinib; PBO, placebo; PYE, patient-years of exposure; TE, treatment-emergent
Figure shows serious infections (SI), venous thromboembolism (VTE) and herpes zoster (HZ) EAIRs.
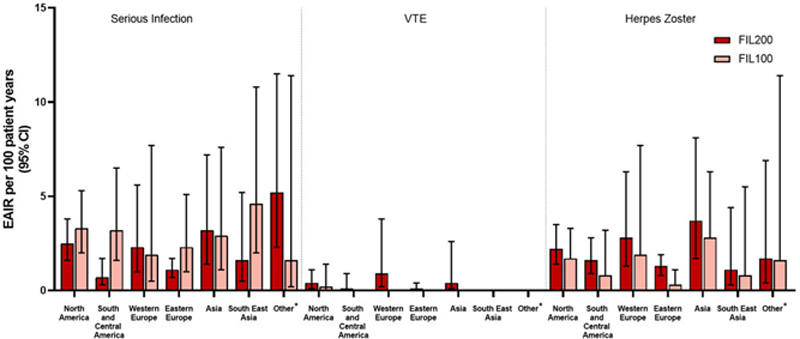
EAIRs for SI were highest in Other for FIL200 and SE Asia for FIL100. While VTE EAIRs were low, pts in 5/7 regions had VTE. HZ EAIRs were highest in Asia.
Conclusion: Although EAIR of TEAEs varied between regions, no consistent trend was reflected in any particular region.
REFERENCES:
[1]Genovese et al. JAMA . 2019;322:315–25.
[2]Westhovens et al. Ann Rheum Dis . 2021; online first.
[3]Combe et al. Ann Rheum Dis . 2021; online first.
Disclosure of Interests: Bernard Combe Speakers bureau: BMS; Eli Lilly & Co.; Gilead Sciences, Inc.; MSD; Pfizer; Roche-Chugai; and UCB, Consultant of: AbbVie; Eli Lilly & Co.; Gilead Sciences, Inc.; Janssen; Pfizer; Roche-Chugai; and Sanofi, Grant/research support from: Novartis, Pfizer, and Roche-Chugai, Tsukasa Matsubara Speakers bureau: Pfizer Japan, Nichi-Iko, Astellas, Meiji Seika, Bristol-Myers Squibb, AbbVie GK, Janssen, Chugai, Eisai, AYUMI, Alena Pechonkina Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., YingMeei Tan Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Zhaoyu Yin Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Jaehyung Hong Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Robin Besuyen Shareholder of: Galapagos, BV, Employee of: Galapagos, BV, Antonio Gomez-Centeno Speakers bureau: AbbVie, Bristol-Myers Squibb, Eli Lilly & Co., Gebro, Janssen, Menarini, Merck Sharp & Dohme, Pfizer, Roche, Rubio, Sanofi, and UC, Consultant of: AbbVie, Biogen, Bristol-Myers Squibb, Celgene, Eli Lilly & Co., Gebro, Gilead Sciences, Inc., Hospira, Merck Sharp & Dohme, Pfizer, Roche, Rubio, Sandoz, Sanofi, Grant/research support from: Boehringer Ingelheim, Celltrion, Eli Lilly & Co., Galapagos NV, Gilead Sciences, Inc., Novartis, Pfizer, Roche, Sanofi, UCB, YL Biologics, Maya H Buch Speakers bureau: AbbVie; Eli Lilly and Company; Gilead Sciences, Inc.; Merck-Serono; Pfizer; Roche; Sandoz; Sanofi; and UCB, Consultant of: AbbVie; Eli Lilly and Company; Gilead Sciences, Inc.; Merck-Serono; Pfizer; Roche; Sandoz; Sanofi; and UCB, Grant/research support from: AbbVie; Eli Lilly and Company; Gilead Sciences, Inc.; Merck-Serono; Pfizer; Roche; Sandoz; Sanofi; and UCB