fetching data ... 
Background: The Janus kinase-1 preferential inhibitor filgotinib (FIL) improved rheumatoid arthritis (RA) signs and symptoms in phase (P)3 trials. 1–3 RA elevates cardiovascular disease risk; statins are used to reduce risk.
Objectives: To assess safety of statin and filgotinib coadministration across the clinical program.
Methods: Patients (pts) meeting 2010 ACR/EULAR RA criteria in P2 DARWIN 1–2 (D1–2; NCT01888874, NCT01894516), P3 FINCH 1–3 (F1–3; NCT02889796, NCT02873936, NCT02886728), and long-term extensions DARWIN 3 and FINCH 4 (D3, F4; NCT02065700, NCT03025308) receiving FIL 100 mg (FIL100) QD, FIL 200 mg QD (FIL200), adalimumab (ADA), methotrexate (MTX), or placebo (PBO) were included. Events related to statin use were analysed as exposed by treatment received. N and % were provided.
Week (W)12 PBO-controlled safety analysis included pts receiving FIL100, FIL200, or PBO for ≤12W (D1–2, F1–2); as-treated safety analysis included pts receiving long-term FIL100 QD (n=1647), FIL200 QD (n=2267), ADA (n=325), MTX (n=416), or PBO (n=781) (D1–3, F1–4); P3 as-randomised analysis included data up to W52 (F1–3) per assigned treatment.
Results: In each arm, similar proportions of pts took statins at baseline (9.4%–11.9%); initiation during study was low (1.2%–6.8%). Through W12 in PBO-controlled analysis, mean creatine phosphokinase (CPK;
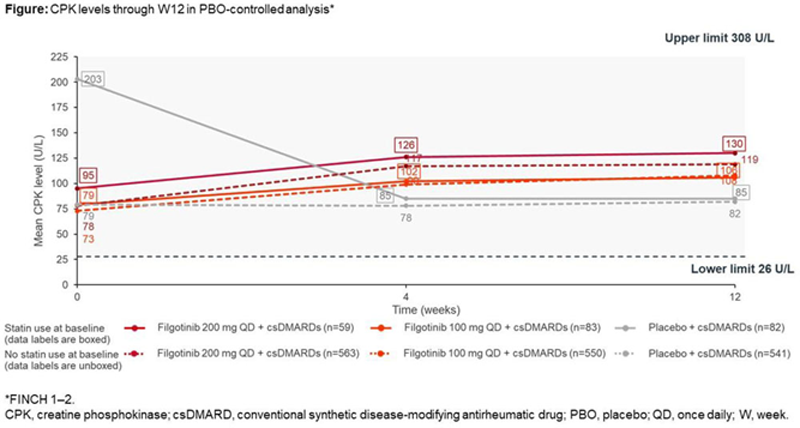
Mean baseline ALT and AST levels were 20–23 and 20–22 U/L, respectively; at W12, ALT and AST ranged from 22–24 and 20–25 U/L, respectively. Graded CPK, ALT, and AST elevations are in
Graded laboratory abnormalities at week 12 by baseline statin use in PBO-controlled analysis
| Concomitant | None | |||||
|
FIL200
|
FIL100
|
PBO
| FIL200 (n=709 ) |
FIL100
|
PBO
|
|
| CPK increased* | 59 | 82 | 81 | 562 | 549 | 537 |
| G1 (≤2.5×ULN) | 10 (16.9) | 13 (15.9) | 6 (7.4) | 71 (12.6) | 47 (8.6) | 18 (3.4) |
| G2 (>2.5 to 5×ULN) | 3 (5.1) | 0 | 0 | 6 (1.1) | 2 (0.4) | 3 (0.6) |
| G3 (>5 to 10×ULN) | 0 | 0 | 0 | 1 (0.2) | 0 | 3 (0.6) |
| G4 (>10×ULN) | 0 | 0 | 0 | 1 (0.2) | 2 (0.4) | 0 |
| AST increased** | 68 | 94 | 92 | 708 | 692 | 684 |
| G1 (≤3.0×ULN) | 9 (13.2) | 11 (11.7) | 7 (7.6) | 97 (13.7) | 79 (11.4) | 60 (8.8) |
| G2 (>3.0 to 5.0×ULN) | 0 | 0 | 0 | 3 (0.4) | 2 (0.3) | 3 (0.4) |
| G3 (>5.0 to 20.0×ULN) | 0 | 1 (1.1) | 0 | 2 (0.3) | 0 | 0 |
| G4 (>20.0×ULN) | 0 | 0 | 0 | 0 | 0 | 0 |
| ALT increased** | 68 | 94 | 92 | 708 | 692 | 684 |
| G1 (≤3.0×ULN) | 13 (19.1) | 14 (14.9) | 13 (14.1) | 98 (13.8) | 92 (13.3) | 72 (10.5) |
| G2 (>3.0 to 5.0×ULN) | 0 | 2 (2.1) | 0 | 10 (1.4) | 5 (0.7) | 6 (0.9) |
| G3 (>5.0 to 20.0×ULN) | 0 | 0 | 0 | 1 (0.1) | 0 | 1 (0.1) |
| G4 (>20.0×ULN) | 0 | 0 | 0 | 0 | 0 | 0 |
Data are n (%). Grading per Common Terminology Criteria for Adverse Events v4.03
*FINCH 1–2
**DARWIN 1–2, FINCH 1–2
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CPK, creatine phosphokinase; csDMARD, conventional synthetic disease-modifying antirheumatic drug; FIL200/100, filgotinib 200/100 mg + csDMARDs; Grade, G; PBO, placebo; ULN, upper limit of normal.
In the long-term as-treated analysis, 1 (0.5%)/6 (3.2%)/0/0/0 treatment-emergent adverse events (AE) of myalgia occurred in pts on statins at baseline receiving FIL200/FIL100/ADA/MTX/PBO and in 12 (0.6%)/8 (0.5%)/3 (1.0%)/2 (0.5%)/1 (0.1%) pts not on statins. Muscle spasms occurred in 2 (0.9%)/3 (1.6%)/1 (3.2%)/0/1 (1.1%) pts on statins at baseline receiving FIL200/FIL100/ADA/MTX/PBO and 21 (1.0%)/8 (0.5%)/0/3 (0.8%)/1 (0.1%) pts not on statins at baseline. One patient not on statins receiving FIL200 reported rhabdomyolysis. For all treatment arms in P3 as-randomised analysis, mean LDL and HDL increased similarly from baseline (108–110 and 56–59 mg/dL, respectively) to W52 (119–130 and 59–71 mg/dL, respectively).
Conclusion: No increases in statin-induced AEs such as muscle or liver toxicities occurred with statins and filgotinib coadministration; results are supported by a drug-drug interaction study. 4 Mean LDL and HDL increased at W52 in all treatment arms.
REFERENCES:
[1]Genovese et al. JAMA. 2019;322:315–25.
[2]Westhovens et al. Ann Rheum Dis . 2021; online first.
[3]Combe et al. Ann Rheum Dis. 2021; online first.
[4]Anderson et al. EULAR 2021 abstract.
Disclosure of Interests: Peter C. Taylor Consultant of: AbbVie, Biogen, Eli Lilly, Fresenius, Galapagos, Gilead, GlaxoSmithKline, Janssen, Nordic Pharma, Pfizer, Roche, BMS, Sanofi, Celltrion, and UCB, Grant/research support from: Celgene, Eli Lilly, Galapagos, and Gilead, Christina Charles-Schoeman Consultant of: Gilead, Pfizer, and Regeneron-Sanofi, Grant/research support from: AbbVie, Bristol-Myers Squibb and Pfizer Inc, Muhsen Alani Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Mona Trivedi Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Vanessa Castellano Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Iyabode Tiamiyu Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Deyuan Jiang Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Lei Ye Shareholder of: Gilead Sciences, Inc., Employee of: Gilead Sciences, Inc., Sander Strengholt Shareholder of: Galapagos BV, Employee of: Galapagos BV, Michael Nurmohamed Speakers bureau: AbbVie, Bristol-Myers Squibb, Eli Lilly, Roche, and Sanofi, Consultant of: AbbVie, Celgene, Celltrion, Eli Lilly, Janssen, and Sanofi, Grant/research support from: AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, MSD, Mundipharma, Novartis, Pfizer, Roche, and Sanofi, Gerd Rüdiger Burmester Speakers bureau: AbbVie, Eli Lilly, Pfizer, and Gilead Sciences, Inc., Consultant of: AbbVie, Eli Lilly, Pfizer, and Gilead Sciences, Inc.