fetching data ... 
Background: The efficacy of ixekizumab (IXE) in biologic-naïve patients with radiographic axial spondyloarthritis (r-axSpA) has been previously presented using traditional axSpA outcome measures, such as BASDAI and ASAS.
Objectives: In patients with active r-axSpA, to assess the analgesic efficacy of IXE as it relates to patient-reported and objective measures of inflammation.
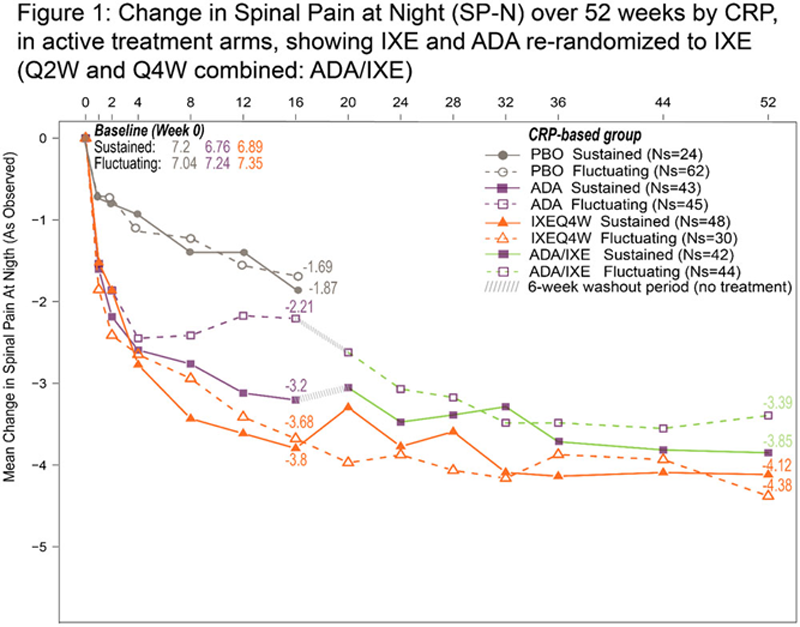
Methods: The Phase III COAST-V (NCT02696785) multi-center, randomized, double-blind, placebo (PBO)-controlled and active reference arm with adalimumab (ADA) trial investigated the efficacy of IXE in 341 patients (pts) with active r-axSpA for 52 weeks (W). Pts were initially randomized to IXEQ4W, IXEQ2W, PBO, and ADAQ2W. At W16, pts assigned to PBO and ADA were re-randomized to IXEQ2W or Q4W. Changes in spinal pain at night (SP-N) and spinal pain were measured at each study visit and analysed while controlling for CRP levels or mean of BASDAI questions 5 & 6 (Q5: Duration and Q6: Intensity of morning stiffness). Observed data analyses are presented for each group stratified by treatment arm and compared to PBO. In the initial analysis, pts were categorized into 2 sub-groups defined as “Sustained” and “Fluctuating” depending on: CRP <5 mg/L W4-16 vs. CRP ≥5 mg/L at any point beyond W4 between weeks 4-16 respectively. In a second analysis, pts were categorized based on BASDAI Q5/6 improvement: “Sustained” if ≥2-pt improvement W12-16 vs. “Fluctuating” if <2-pt improvement at any point beyond W12 between W12-16.
Results: Between W0 and W16, pts treated (tx) with IXEQ4W experienced greater reduction in SP-N than pts tx with ADA, in both CRP sustained and fluctuating groups (
Change in Pain Outcome at baseline, week 16 and week 52 by Inflammation Status as assessed by BASDAI or CRP levels for patients receiving placebo (PBO), adalimumab (ADA), and ixekizumab every 4 weeks (IXE Q4W)
| Change from baseline | ||||||||||
| PBO | ADA | IXEQ4W | ||||||||
| baseline | Week 16
| Week 52
| baseline | Week 16
| Week 52
| baseline | Week 16
| Week 52
|
||
| Spinal pain | BASDAI Q5/6 sustained | 7.54 | -3.33 | -4.65 | 7.21 | -4.07 | -4.5 | 7.4 | -4.52 | -4.94 |
| BASDAI Q5/6 fluctuating | 7.37 | -1.32 | -2.82 | 6.76 | -1.2 | -2.24 | 6.97 | -1.3 | -2.52 | |
| CRP sustained | 7 | -1.53 | -1.93 | 6.83 | -2.9 | -3.6 | 7.23 | -3.57 | -4.21 | |
| CRP fluctuating | 7.51 | -1.96 | -3.63 | 7.28 | -2 | -2.89 | 7.24 | -2.91 | -3.93 | |
| Spinal pain at night | BASDAI Q5/6 sustained | 7.12 | -3.21 | -4.61 | 7.26 | -4.63 | -4.92 | 7.12 | -4.73 | -4.91 |
| BASDAI Q5/6 fluctuating | 7.05 | -1.15 | -2.88 | 6.6 | -1.2 | -2.49 | 7.03 | -2.17 | -2.92 | |
| CRP sustained | 7.2 | -1.87 | -2.27 | 6.76 | -3.2 | -3.85 | 6.89 | -3.8 | -4.12 | |
| CRP fluctuating | 7.04 | -1.69 | -3.6 | 7.24 | -2.21 | -3.39 | 7.35 | -3.68 | -4.38 | |
Conclusion: IXE reduced SP-N and spinal pain irrespective of CRP or morning stiffness. Additionally, pts treated with ADA re-randomized to IXE experienced a further reduction in SP-N and spinal pain. Collectively, these results support the additive benefits of IXE in reducing pain above measurable effects on inflammation.
Acknowledgements: The authors would like to thank Eglantine Julle-Daniere for writing and editorial contributions
Disclosure of Interests: Kurt de Vlam Speakers bureau: Eli Lilly, Novartis, Pfizer, Paid instructor for: Celgene, Amgen, Consultant of: Elil Lillyn Novartis, UCB, Galapagos, Sandoz, Pfizer, Grant/research support from: Celgene, Gaia Gallo Shareholder of: Eli Lilly, Employee of: Eli Lilly, Philip J Mease Speakers bureau: AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer, UCB, Consultant of: AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, Sun, UCB, Grant/research support from: AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Galapagos, Janssen, Novartis, Pfizer, Sun, UCB, Proton Rahman Speakers bureau: AbbVie, Amgen, BMS, Celgene, Eli Lilly, Janssen, Merck, Novartis, Pfizer, UCB, Consultant of: AbbVie, Amgen, BMS, Celgene, Eli Lilly, Janssen, Merck, Novartis, Pfizer, UCB, Grant/research support from: Janssen, Novartis, Venkatesh Krishnan Shareholder of: Eli Lilly, Employee of: Eli Lilly, David Sandoval Shareholder of: Eli Lilly, Employee of: Eli Lilly, Chen-Yen Lin Shareholder of: Eli Lilly, Employee of: Eli Lilly, Rebecca Bolce Shareholder of: Eli Lilly, Employee of: Eli Lilly, Philip G Conaghan Consultant of: personal fees from: AbbVie, AstraZeneca, BMS, Eli Lilly, EMD Serono, Flexion Therapeutics, Galapagos, Gilead, Novartis, Pfizer