fetching data ... 
Background: Tyrosine kinase 2 (TYK2) is an intracellular kinase that mediates interleukin (IL)-23, IL-12, and interferon (IFN)α/β signaling. Deucravacitinib is a novel, oral, selective inhibitor of TYK2 acting via binding to the TYK2 regulatory domain. 1 Phase 2 results showed deucravacitinib was efficacious and well tolerated versus placebo in patients with moderate to severe plaque psoriasis or active psoriatic arthritis. 2,3 No herpes zoster infections, opportunistic infections, thromboembolic events, or hematologic or lipid abnormalities characteristic of Janus kinase (JAK) 1−3 inhibitors were reported in the Phase 2 trials. 2,3
Objectives: To compare the efficacy and safety of deucravacitinib versus placebo and apremilast in plaque psoriasis.
Methods: This Phase 3, double-blinded, 52-week study (NCT03624127) randomized patients with moderate to severe plaque psoriasis (BSA ≥10%, PASI ≥12, sPGA ≥3) to deucravacitinib 6 mg once daily, placebo, or apremilast 30 mg twice daily (2:1:1). Patients receiving placebo were switched to deucravacitinib at Week 16; apremilast-treated patients not achieving PASI 50 at Week 24 were switched to deucravacitinib. Coprimary endpoints were PASI 75 and sPGA 0/1 response versus placebo at Week 16. Key secondary endpoints included superiority versus apremilast, assessed via multiple measures.
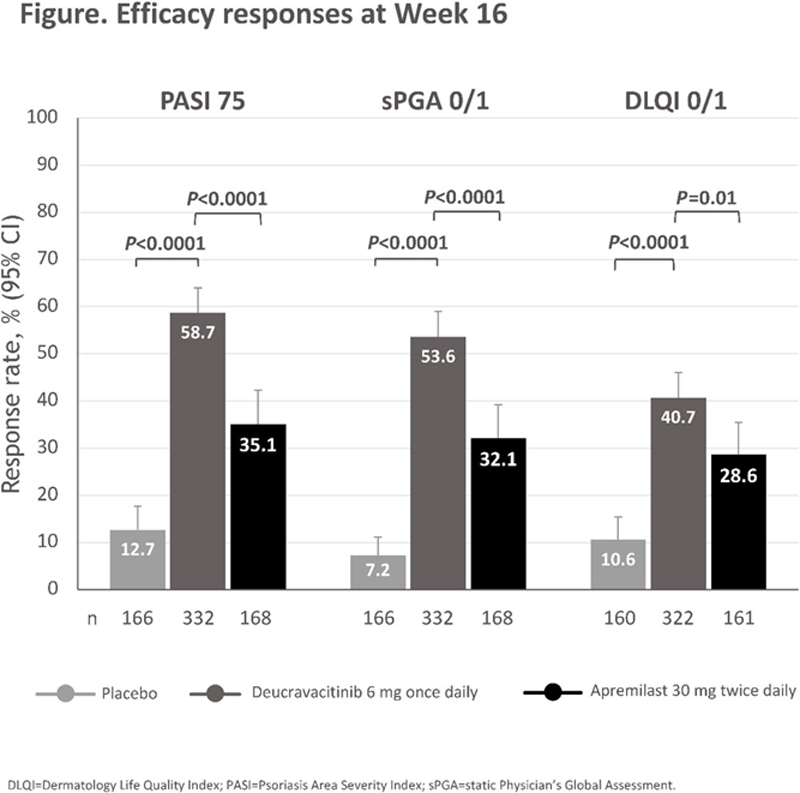
Results: 666 patients were randomized. Demographic and baseline disease characteristics were balanced across groups; mean age was 46.1 years, mean disease duration was 17.3 years, 18.2% of patients had psoriatic arthritis at baseline, and 38.9% had previously used biologic therapy. Mean BSA involvement at baseline was 26.3%, mean PASI was 21.4, and the percentage with severe sPGA (score=4) at baseline was 21.2%. Significantly greater proportions of patients in the deucravacitinib versus placebo and apremilast arms achieved PASI 75 (58.7% vs 12.7% vs 35.1%, respectively;
P
<0.0001) and sPGA 0/1 (53.6% vs 7.2% vs 32.1%, respectively;
P
<0.0001) response at Week 16 (
Summary of adverse events (AEs) through Week 16
| Patients, n (% ) |
Deucravacitinib
|
Placebo
|
Apremilast
|
| Any AEs | 176 (53.0) | 70 (42.4) | 93 (55.4) |
| Severe AEs | 5 (1.5) | 7 (4.2) | 5 (3.0) |
| Serious AEs | 7 (2.1) | 9 (5.5) | 4 (2.4) |
| AEs leading to treatment discontinuation | 6 (1.8) | 7 (4.2) | 10 (6.0) |
| Most common AEs (≥5% in any arm ) | |||
| Nasopharyngitis | 21 (6.3) | 7 (4.2) | 14 (8.3) |
| Upper respiratory tract infection | 21 (6.3) | 6 (3.6) | 3 (1.8) |
| Headache | 16 (4.8) | 5 (3.0) | 17 (10.1) |
| Diarrhea | 13 (3.9) | 6 (3.6) | 17 (10.1) |
| Nausea | 7 (2.1) | 4 (2.4) | 19 (11.3) |
Conclusion: Deucravacitinib demonstrated superiority versus placebo and apremilast across multiple efficacy endpoints in patients with moderate to severe plaque psoriasis, and was generally well tolerated. Overall, the efficacy and safety profile of deucravacitinib was consistent with that observed in the Phase 2 plaque psoriasis and psoriatic arthritis trials. 2,3
REFERENCES:
[1]Burke JR et al. Sci Transl Med. 2019;11:1-16.
[2]Papp K et al. N Engl J Med. 2018;379:1313-21.
[3]Mease PJ et al. Presented at: Annual Scientific Meeting of the American College of Rheumatology; November 5-9, 2020; Virtual meeting.
Acknowledgements: This study was sponsored by Bristol Myers Squibb. Professional medical writing assistance was provided by Peloton Advantage, LLC, an OPEN Health company, and funded by Bristol Myers Squibb.
Disclosure of Interests: April Armstrong Consultant of: Grants and personal fees from AbbVie, Bristol Myers Squibb, Eli Lilly, Janssen, Leo Pharma, Novartis; Personal fees from Boehringer Ingelheim/Parexel, Celgene, Dermavant, Genentech, GlaxoSmithKline, Menlo Therapeutics, Merck, Modernizing Medicine, Ortho Dermatologics, Pfizer, Regeneron, Sanofi Genzyme, Science 37, Sun Pharma, Valeant, Grant/research support from: Grants: Dermira, Kyowa Hakko Kirin, and UCB, outside the submitted work; Grants and personal fees from AbbVie, Bristol Myers Squibb, Eli Lilly, Janssen, Leo Pharma, Novartis, Melinda Gooderham Shareholder of: Speakers bureau, consultant, investigator/advisor: AbbVie, Akros, Amgen, Arcutis, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Dermira, Eli Lilly, Galderma, GlaxoSmithKline, Incyte, Janssen, Kyowa Hakko Kirin, Leo Pharma, Merck, MedImmune, Novartis, Pfizer, Regeneron, Roche, Sanofi Genzyme, Takeda, UCB, Valeant, Richard B. Warren Consultant of: AbbVie, Almirall, Amgen, Boehringer Ingelheim, Celgene, Janssen, Leo Pharma, Eli Lilly, Novartis, Pfizer, Sanofi, Xenoport, UCB, Grant/research support from: AbbVie, Almirall, Amgen, Celgene, Janssen, Eli Lilly, Leo Pharma, Novartis, Pfizer, UCB, Kim Papp Speakers bureau: AbbVie, Amgen, Astellas, Celgene, Eli Lilly, Galderma, Janssen, Kyowa Hakko Kirin, Leo Pharma, Merck Sharp & Dohme, Novartis, Pfizer, Valeant, Consultant of: Scientific officer/steering committee/advisory board: AbbVie, Akros, Amgen, Anacor, Astellas, Baxter, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Dow Pharma, Eli Lilly, Galderma, Janssen, Kyowa Hakko Kirin, Merck Sharp & Dohme, Merck Serono, Novartis, Pfizer, Regeneron, Sanofi-Aventis/Genzyme, Valeant, Grant/research support from: AbbVie, Akros, Allergan, Amgen, Anacor, Arcutis, AstraZeneca, Baxalta, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Coherus, Dermira, Dow Pharma, Eli Lilly, Galderma, Genentech, GlaxoSmithKline, Janssen, Kyowa Hakko Kirin, Leo Pharma, MedImmune, Meiji Seika Pharma, Merck Serono, Novartis, Pfizer, Regeneron, Roche, Sanofi-Aventis/Genzyme, Takeda, UCB, Valeant;
Consultant: AbbVie, Akros, Amgen, Arcutis, Astellas, AstraZeneca, Baxalta, Baxter, Boehringer Ingelheim, Bristol Myers Squibb, CanFite, Celgene, Coherus, Dermira, Dow Pharma, Eli Lilly, Forward Pharma, Galderma, Genentech, Janssen, Kyowa Hakko Kirin, Leo Pharma, Meiji Seika Pharma, Merck Sharp & Dohme, Merck Serono, Mitsubishi Pharma, Novartis, Pfizer, Regeneron, Roche, Sanofi-Aventis/Genzyme, Takeda, UCB, Valeant; Honoraria: AbbVie, Akros, Amgen, Baxter, Boehringer Ingelheim, Celgene, Coherus, Eli Lilly, Forward Pharma, Galderma, GlaxoSmithKline, Janssen, Kyowa Hakko Kirin, Merck Sharp & Dohme, Merck Serono, Novartis, Pfizer, Takeda, UCB, Valeant, Bruce Strober Speakers bureau: AbbVie, Janssen, Eli Lilly, Ortho Dermatologics, Consultant of: Honoraria or consultation fees: AbbVie, Almirall, Amgen, Arena, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Dermavant, Dermira, Eli Lilly, GSK, Janssen, Kyowa Hakko Kirin, Leo Pharma, Medac, Meiji Seika Pharma, Novartis, Ortho Dermatologics, Pfizer, Regeneron, Sanofi-Genzyme, Sun Pharma, UCB; Scientific Director (consulting fee): Corrona Psoriasis Registry; Investigator: AbbVie, Corrona Psoriasis Registry, Dermavant, Dermira., Diamant Thaçi Paid instructor for: Lectures: AbbVie, Almirall, Amgen, DS-Pharma, Janssen, Leo Pharma, MSD, Novartis, Pfizer, Roche-Posay, Sandoz-Hexal, Sanofi, Target-Solution, UCB; Scientific advisory board: AbbVie, Amgen, Celgene, DS Pharma, Eli Lilly, Galapagos, Janssen-Cilag, Leo Pharma, Morphosis, MSD Novartis, Pfizer, Sandoz, Sanofi, UCB., Consultant of: Consultant: AbbVie, Almirall, Celgene, Dignity, Galapagos, Leo Pharma, Maruho, Mitsubishi, Novartis, Pfizer, Xenoport, Grant/research support from: Research support/principal investigator (clinical trials): AbbVie, Almirall, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Chugai, Dermira, DS-Pharma, Eli Lilly, Galderma, GSK, Janssen-Cilag, Leo, MSD, Novartis, Pfizer, Regeneron, Roche, Sandoz-Hexal, Sanofi, UCB, Elizabeth Colston Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, John Throup Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Sudeep Kundu Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Subhashis Banerjee Shareholder of: Bristol Myers Squibb, Employee of: Bristol Myers Squibb, Andrew Blauvelt Consultant of: Scientific adviser and/or clinical study investigator for AbbVie, Aligos, Almirall, Arena, Athenex, Boehringer Ingelheim, Bristol Myers Squibb, Dermavant, Eli Lilly, Evommune, Forte, Galderma, Incyte, Janssen, Leo Pharma, Novartis, Pfizer, Rapt, Regeneron, Sanofi Genzyme, Sun Pharma, UCB Pharma.