fetching data ... 
Background: EQUATOR (NCT03101670) was a Phase 2, double-blind, randomised placebo (PBO)- controlled trial of the preferential Janus kinase 1 inhibitor filgotinib (FIL) for the treatment of psoriatic arthritis (PsA); EQUATOR2 (NCT03320876) is the open-label extension (OLE).
Objectives: This post-hoc analysis assessed the effect of FIL on individual Psoriatic Arthritis Disease Activity Score (PASDAS) components; and the association between PASDAS disease activity (DA) levels and DA levels achieved for each PASDAS component and patient-reported outcomes (PROs) up to OLE Week (Wk) 100.
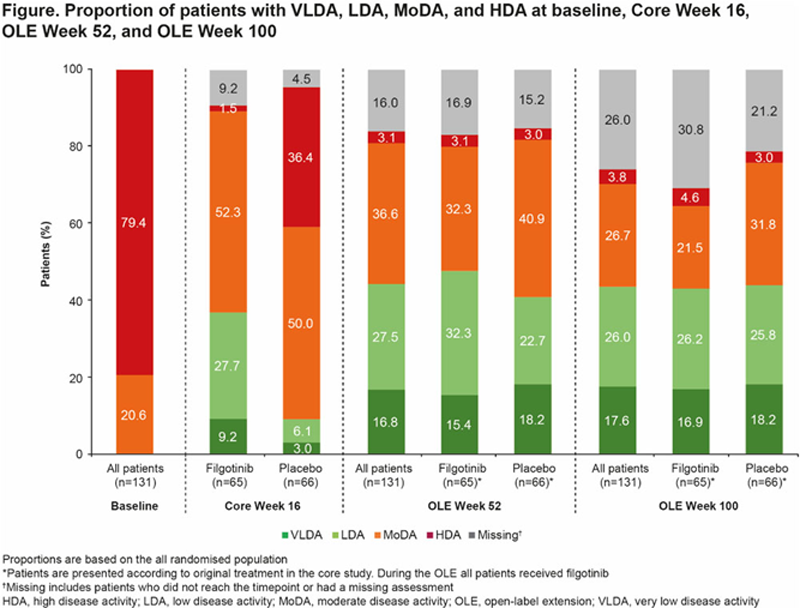
Methods: In EQUATOR, patients with active moderate-to-severe PsA were randomised 1:1 to oral FIL 200 mg or PBO once daily (QD) for 16 wks. 1 At Wk 16, patients could continue into the 304-wk OLE, in which all patients received FIL 200 mg QD. The proportions of patients with PASDAS of very low DA (VLDA; ≤1.9), LDA (>1.9–<3.2), moderate DA (MoDA; ≥3.2–<5.4), and high DA (HDA; ≥5.4) at core Wk 16 and OLE Wk 52 and 100 were assessed. The proportion with improved PASDAS status vs baseline (BL) at OLE Wk 52 and 100 was calculated. Percent change from BL in PASDAS components and PROs were assessed at core Wk 16 and OLE Wk 52 and 100 by PASDAS status (VLDA, LDA, other). Multivariate logistic regression analyses performed cross-sectionally identified PASDAS components and PROs associated with not achieving VLDA or LDA at core Wk 16 and OLE Wk 52 and 100; all analyses were observed cases.
Results: At OLE Wk 52, LDA and VLDA were achieved by 27.5% and 16.8% of randomised patients, respectively (44.3% combined). At OLE Wk 100, LDA and VLDA were achieved by 26.0% and 17.6% of patients (43.6% combined;
Conclusion: The proportion of patients achieving PASDAS VLDA or LDA increased over time and remained stable between OLE Wk 52 and 100. Important factors in determining whether VLDA/LDA was met were PtGDA, PhGDA, and SF-36 PCS, although the low patient numbers is a limitation.
REFERENCES:
[1]Mease P, et al. Lancet . 2018;392:2367–77
Mean % change from baseline in PASDAS components and PROs (observed cases)
|
Core Wk 16 (FIL + PBO groups combined
)
|
OLE Wk 52
|
OLE Wk 100
|
|||||||
| VLDA
| LDA
| Others
| VLDA
| LDA
| Others
| VLDA n=23
| LDA
| Others
|
|
| PhGDA | −93 | −75 | −44 | −94 | −82 | −56 | −96 | −84 | −54 |
| PtGDA | −87 | −69 | −13 | −86 | −58 | −24 | −90 | −57 | −13 |
| Tender joint count 68 | −94 | −80 | −42 | −99 | −84 | −64 | −98 | −87 | −61 |
| Swollen joint count 66 | −99 | −80 | −64 | −99 | −96 | −78 | −99 | −94 | −80 |
| LEI | −100 | −86 | −32 | −96 | −100 | −78 | −100 | −99 | −78 |
| Dactylitis | −100 | −100 | −73 | −100 | −100 | −97 | −100 | −100 | −98 |
| C-reactive protein | −66 | −22 | 17 | 138* | −32 | −25 | −12 | −13 | 24 |
| SF-36 PCS | 53 | 26 | 11 | 33 | 23 | 9 | 47 | 23 | 16 |
| FACIT | 119 | 50 | 32 | 97 | 51 | 34 | 99 | 46 | 36 |
| HAQ-DI | −84 | −68 | −18 | −85 | −51 | −18 | −88 | −45 | −19 |
| PASI | −84 | −66 | −29 | −54 | −59 | −56 | −49 | −76 | −42 |
Components or PRO measures in bold are those for which numerical differences between VLDA and LDA are greatest across timepoints
*Due to outlier (3784)
FACIT, Functional Assessment of Chronic Illness Therapy; HAQ-DI, Health Assessment Questionnaire Disability Index; LEI, Leeds Enthesitis Index; PASI, Psoriasis Area Severity Index; PhGDA, Physician Global Assessment of Disease Activity; PtGDA, Patient Global Assessment of Disease Activity; SF-36 PCS, Short Form-36 physical component summary; (V)LDA, (very) low disease activity
Acknowledgements: EQUATOR and EQUATOR2 were sponsored by Galapagos NV Mechelen, Belgium) and co-funded by Galapagos NV and Gilead Sciences, Inc (Foster City, CA, USA). Benjamin Pett and his team, employees of Galapagos, provided assistance with statistical analyses. Medical writing/editorial support was provided by Debbie Sherwood, BSc, CMPP (Aspire Scientific, Bollington, UK), and was funded by Galapagos NV.
Disclosure of Interests: Laura C Coates Speakers bureau: AbbVie, Amgen, Biogen, Celgene, Eli Lilly, Gilead, Janssen, Medac, Novartis, Pfizer, and UCB, Consultant of: AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Gilead, Janssen, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Amgen, Celgene, Eli Lilly, Novartis, and Pfizer, Philip J Mease Speakers bureau: AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer, and UCB, Consultant of: AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead Sciences, GlaxoSmithKline, Janssen, Novartis, Pfizer, SUN, and UCB, Grant/research support from: AbbVie, Amgen, Bristol Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead Sciences, Janssen, Novartis, Pfizer, SUN, and UCB, Philip Helliwell Paid instructor for: Janssen, Novartis, and Pfizer, Consultant of: Eli Lilly, Filip van den Bosch Consultant of: AbbVie, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Merck, and UCB, Mona Trivedi Shareholder of: Gilead Sciences, Amgen, Employee of: Gilead Sciences, Muhsen Alani Shareholder of: Gilead Sciences, Employee of: Gilead Sciences, Franck Olivier Le Brun Shareholder of: Galapagos, Employee of: Galapagos, Robin Besuyen Shareholder of: Galapagos, Employee of: Galapagos, Lien Gheyle Shareholder of: Galapagos, Employee of: Galapagos, Emilia Gvozdenovic Employee of: Galapagos, Dafna D Gladman Consultant of: AbbVie, Amgen, Bristol Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer, and UCB., Grant/research support from: AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, and UCB.