fetching data ... 
Background: Shoulder pain is common and persistent, with a large socioeconomic burden. Ultrasound (US) scans are used for diagnosing and managing shoulder pain, but the extent to which it informs management and improves outcomes is unknown. A recent retrospective study identified groups with different patterns of US pathologies.
Objectives: To confirm the existence of US-based groups of shoulder pain and determine if US-detected pathology (grouped or individual) predicts outcomes in the context of usual care. Response to local steroid injection was also evaluated.
Methods: This was a 6 month, prospective, single centred, community based, observational cohort study. Inclusion: shoulder pain, ≥18 years, first shoulder US. Exclusion: shoulder surgery, inflammatory arthritis, steroid/physiotherapy in prior 6 weeks. Standardised reporting for 10 US pathologies was employed. Latent class analysis (LCA) identified pathology-based groups. Multiple linear regression analysis explored associations between baseline pathologies, subsequent treatment and 6-month Shoulder Pain and Disability Index (SPADI). Growth mixture modelling (GMM) identified groups with common trajectories of change.
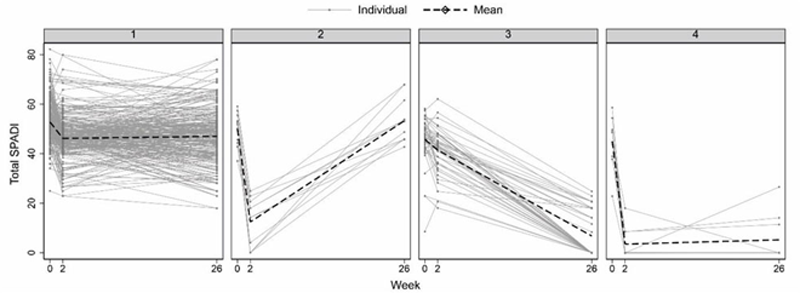
Results: Of 500 patients (mean age 53.6; 52% female), 330 completed follow-up. LCA identified 4 groups: bursitis without acromioclavicular joint degeneration (ACJD) (group 1), bursitis with ACJD (group 2), rotator cuff tear (group 3), no bursitis/tear (group 4). SPADI was higher at baseline for tears (55.1 vs. 49.7-51.3) (overall p=0.005), but groups did not differ at 6 months (p=0.379) (
Conclusion: This is the largest prospective study involving US of symptomatic shoulders, and the first to investigate groups with distinct patterns of US pathologies in predicting outcome. US-based classification of pathology (as groups or individually) did not predict 6-month outcomes with current treatments and there were no differences in short-term response to steroids between groups. The role of routine diagnostic US for shoulder pain needs consideration; it may be useful if evidence-based therapies for specific pathologies are established.
Predictors of SPADI score at 6 months
| Baseline characteristic | Coefficient* (95% CI), p-value |
| Pathology group:Bursitis w/o ACJ degeneration (group 1) | Reference |
| Bursitis with ACJ degeneration (group 2) | 0.08 (-5.15, 5.32), p=0.975 |
| RC tear (group 3) | 5.01 (-1.48, 11.50), p=0.130 |
| No bursitis, no RC tear (group 4) | 1.98 (-4.00, 7.96), p=0.516 |
| Injection at scan | 4.87 (0.40, 9.34), p=0.033 |
| Age, years | -0.01 (-0.17, 0.15), p=0.898 |
| Female | -1.51 (-5.42, 2.40), p=0.448 |
| Symptom duration, months | 0.00 (-0.04, 0.05), p=0.879 |
| Uses arms to rise from chair | 2.65 (-1.50, 6.81), p=0.210 |
| Physiotherapy before baseline | -0.23 (-4.78, 4.31), p=0.920 |
| 1 injection before baseline | 2.35 (-2.87, 7.56), p=0.377 |
| ≥2 injections before baseline | 6.53 (-2.50, 15.57), p=0.156 |
| Total SPADI | 0.62 (0.35, 0.89), p<0.001 |
| Shoulder activity score | -0.59 (-1.15, -0.04), p=0.037 |
| P-SEQ score | -0.20 (-0.46, 0.07), p=0.141 |
| Brief IPQ score | 0.19 (-0.16, 0.54), p=0.298 |
| HADS score | 0.01 (-0.38, 0.41), p=0.947 |
| Constant** | 35.44 (29.50, 41.38), p<0.001 |
*Interpreted as unit difference in Rasch-transformed SPADI score per 1 additional unit of the independent variable **Estimated SPADI at 26 weeks in patients in the reference category for all categorical variables and with mean values for continuous covariates. ACJ=acromioclavicular joint; HADS=hospital anxiety and depression scale; IPQ=illness perception questionnaire; P-SEQ=pain self-efficacy questionnaire; RC=rotator cuff; SPADI=shoulder pain and disability index
Trajectories of total SPADI over time by the pathology groups found and response to injections
Acknowledgements: This research was funded by the National Institute for Health Research (NIHR) Leeds Biomedical Research Centre (BRC) and by a NIHR Doctoral Research Fellowship (GT; DRF-2016-09-159). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. This study was also part-funded through the Arthritis Research UK Leeds Experimental Osteoarthritis Treatment Centre (20083).
Disclosure of Interests: None declared