fetching data ... 
Background: Hydroxychloroquine (HCQ) is an extensively used drug in immune-mediated diseases (IMID). Despite its general safety, HCQ can cause serious toxicity such as heart conduction disorders. Atrioventricular block (AVB) is an underrecognized adverse effect that can potentially cause significant morbidity and mortality.
Objectives: To study incidence, presentation, and characteristics of HCQ-induced AVB in IMID.
Methods: Open-label single center study of 293 patients with IMID treated with HCQ for at least 3 months. Electrocardiograms were analyzed at baseline and during HCQ treatment. In addition, a comparative study between patients with and without AVB was conducted.
Results: We studied 293 patients (270 women/ 23 men; mean age 59.7±14.7 years). Underlying IMID were Systemic Lupus Erythematosus (SLE) (n=109, 40.6%); undifferentiated connective-tissue disease (n=70, 23.9%), Sjögren’s syndrome (SS) (n=70, 23.9%), antiphospholipid syndrome (n=31,10.6%) and other IMID (n=13, 4.4%). HCQ was used for 4.1±3.5 years.
After 11.8±8.9 years of follow-up (HCQ mean cumulative dose: 979.7±272.1 g). AVB was observed in 19 out of 293 (6.5%) patients: 16 (84.2%) were first-degree AVB and 3 (15.8%) complete AVB. 4 (21.2%) patients with AVB were treated with a permanent pacemaker.
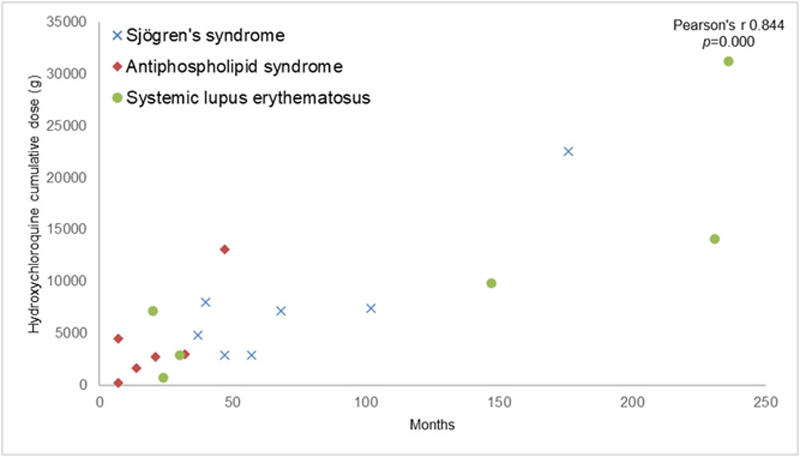
Presentation of atrioventricular block according to hydroxychloroquine incidence rate and treatment duration is shown in
Presentation of atrioventricular block according to hydroxychloroquine incidence rate and treatment duration.
A comparative study between patients with and without AVB was performed (
Other HCQ adverse effects were retinopathy (n=16, 5.4%), gastrointestinal alterations (n=14, 4.8%), cutaneous alterations (n=14, 4.8%), allergic reactions (n=4, 1.4%) and myopathy (n=1, 0.3%).
Conclusion: AVB was observed in 6.5% of patients with IMID treated with HCQ. Most AVB were first-degree AVB. HCQ increased the risk of developing an AVB in patients with IMID regardless of HCQ cumulative dose or underlying disease duration. Older patients with diabetes mellitus had a higher risk of developing an AVB.
Comparative study between patients with and without AVB.
| with AVB
| without AVB
| p | |
| General features at HCQ onset | |||
| Age, years mean±SD | 57.4±14.5 | 46.4±16.8 | 0.014 |
| Female, n (%) | 17(89.5) | 239(87.4) | 0.877 |
| Hypertension, n (%) | 14 (73.7) | 149 (54.4) | 0.118 |
| Dyslipemia, n (%) | 11 (58.9) | 117 (42.7) | 0.265 |
| Diabetes Mellitus, n (%) | 5 (26.3) | 24 (8.7) | 0.033 |
| Renal impairment, n (%) | 5 (26.3) | 29 (10.7) | 0.073 |
| Ischemic cardiopathy, n (%) | 2 (10.5) | 11 (3.9) | 0.228 |
| CRP, mg/dL median [IQR] | 0.3 [0.1-0.5] | 0.4 [0.3-0.8] | 0.343 |
| ESR, mm/h median [IQR] | 17.0 [15.0-22.3] | 13.0 [7.0-29.5] | 0.206 |
| Data at last visit (11.8±8.9 years of follow-up) | |||
| IMID duration, years mean±SD | 11.8±8.9 | 14.3±10.3 | 0.288 |
| # Use of other cardiotoxic drugs, n (%) | 2 (10.5) | 11 (4.0) | 0.723 |
| HCQ cumulative dose, g mean±SD | 813.2±206.0 | 996.3±266.9 | 0.527 |
# (beta blockers, calcium channel blockers, tricyclic drugs, other AVB inducers)
Disclosure of Interests: Alba Herrero-Morant: None declared, Adrián Margarida-de Castro: None declared, Raquel Pérez-Barquín: None declared, Jon Zubiaur-Zamacola: None declared, Miguel Á. González-Gay Speakers bureau: AbbVie, Pfizer, Roche, Sanofi, Lilly, Celgene and MSD, Grant/research support from: AbbVie, MSD, Jansen and Roche, Ricardo Blanco Speakers bureau: AbbVie, Pfizer, Roche, Bristol-Myers, Janssen, Sanofi, Lilly and MSD, Grant/research support from: AbbVie, MSD, and Roche