fetching data ... 
Background: Subcutaneous (SC) CT-P13 is the first and only subcutaneous formulation of infliximab (IFX) approved by the EMA. 1 In the pivotal study (NCT03147248), non-inferiority of SC IFX to intravenous (IV) was demonstrated in rheumatoid arthritis (RA) patients using 28-joint Disease Activity Score (DAS28) C-reactive protein (CRP) improvement at Week 22, with a statistically significant treatment difference of 0.27 (95% CI 0.02, 0.52) favoring the SC versus the IV arm. 2,3 At Week 30, numerical differences in efficacy outcomes were shown between SC and IV IFX favoring SC IFX. IV group patients switched to SC IFX by Week 30, and the difference between the groups was reduced at Week 54. 2
Objectives: To investigate whether there was a statistically significant difference between SC and IV IFX at Weeks 30 and 54 in the phase 3 pivotal study of CT-P13 SC using conservative missing imputation methods.
Methods: Patients with active RA who had an inadequate response to MTX received IV IFX 3mg/kg at Weeks 0 and 2 for induction and were randomized at a 1:1 ratio to receive SC IFX 120mg every 2 weeks or IV 3mg/kg every 8 weeks thereafter for maintenance. Patients who were randomized to receive IV IFX switched to SC at Week 30. In this post-hoc analysis, non-responder imputation (NRI) and last observation carried forward (LOCF) methods were used to investigate whether the difference in efficacy outcomes between SC and IV IFX at Weeks 30 and 54 was statistically significant. Assessments included EULAR (CRP/ESR)/ACR response; remission rate and low disease activity (LDA) rate based on DAS28 (CRP/ESR), Clinical Disease Activity Index (CDAI) and Simplified Disease Activity Index (SDAI); Boolean remission rate; and the proportion of patients achieving a minimal clinically important difference (MCID) in Health Assessment Questionnaire (HAQ).
Results: Of the 343 randomized patients, 165 patients who received SC IFX and 174 patients who received IV IFX from the efficacy population were included in the analysis. There was a statistically significant difference in SC IFX compared to IV treated patients at Week 30 using both NRI and LOCF methods in almost all the clinical variables. However, the difference in efficacy outcomes between SC IFX and IV was reduced at Week 54 after the IV group switched to SC. This supports the improved efficacy of SC IFX at Week 30. Some of the key results (EULAR [CRP] responses, LDA rates based on DAS28 [CRP], CDAI, and SDAI) were presented in
Comparison of clinical outcomes between SC IFX and IV IFX in patients with active rheumatoid arthritis.
*P<0.05.
P-value for difference in proportion between SC and IV treatment group was obtained by asymptotic Wald test.
Low disease activity based on DAS28 (CRP) (< 3.2), CDAI (eatment group AI (≤ 11.0).
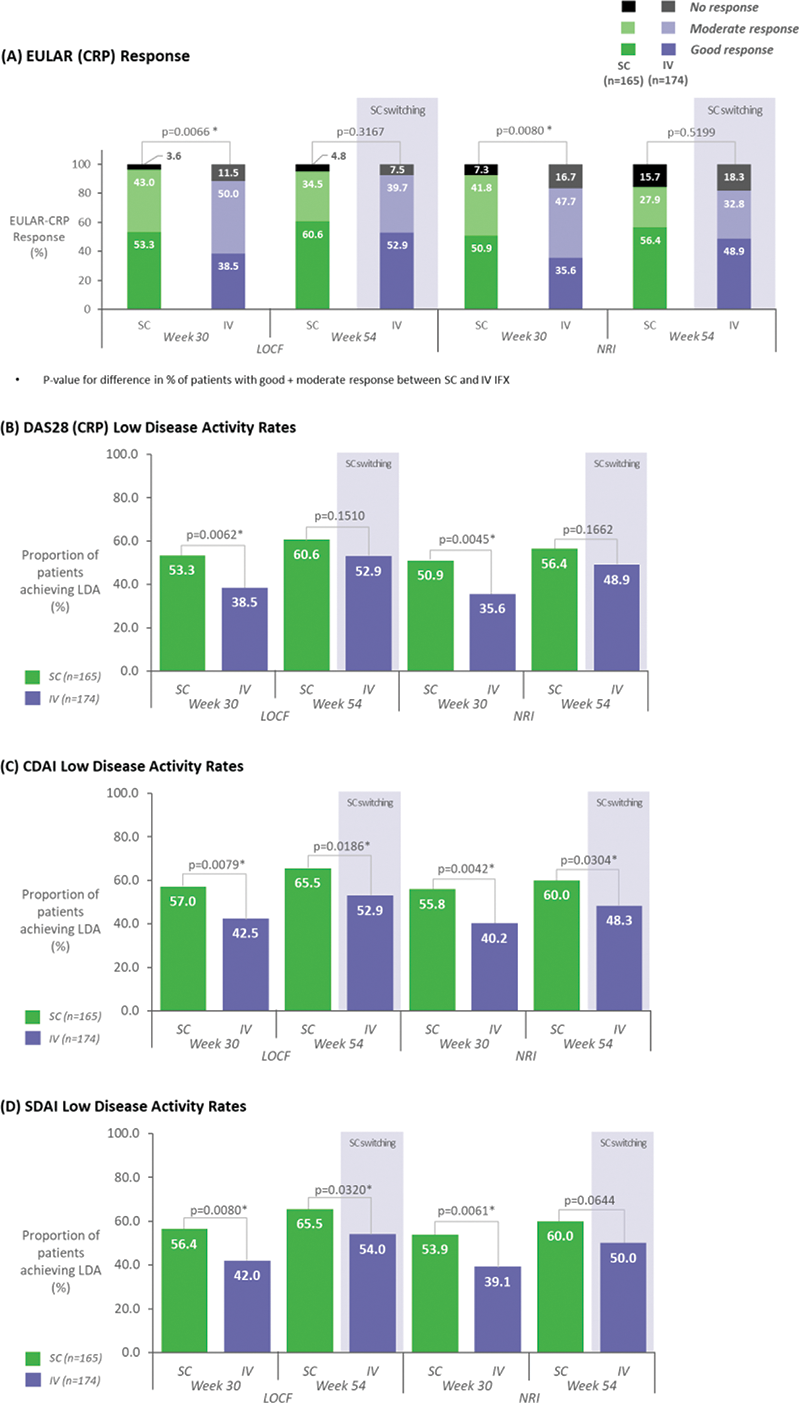
Conclusion: Statistical analyses using conservative missing imputation methods showed significantly greater improvements in clinical outcomes with SC IFX compared to IV at Week 30 in patients with RA. Between-group differences was reduced at Week 54, suggesting improved responses after switching from IV to SC.
REFERENCES:
[1]Remsima summary of product characteristics.
[2]Westhovens R, Wiland P, Zawadzki M, et al. Efficacy, pharmacokinetics and safety of subcutaneous versus intravenous CT-P13 in rheumatoid arthritis: a randomized phase I/III trial. Rheumatology (Oxford). 2021;60(5):2277-2287.
[3]Combe B, Allanore Y, Alten R, et al. Comparative efficacy of subcutaneous (CT-P13) and intravenous infliximab in adult patients with rheumatoid arthritis: a network meta-regression of individual patient data from two randomised trials. Arthritis Res Ther. 2021;23(1):119.
Disclosure of Interests: Arnaud Constantin Speakers bureau: Abbvie, Amgen, Boehringer, Celltrion, Galapagos, Janssen, Lilly, Novartis, Sanofi, UCB, Consultant of: Abbvie, Amgen, Boehringer, Celltrion, Galapagos, Janssen, Lilly, Novartis, Sanofi, UCB, Roberto Caporali Speakers bureau: Abbvie, Amgen, BMS, Celltrion, Galapagos, Lilly, Pfizer, Fresenius-Kabi, MSD, UCB, Roche,Janssen, Novartis, Sandoz, Consultant of: Abbvie, Amgen, BMS, Celltrion, Galapagos, Lilly, Pfizer, MSD, UCB, Janssen, Novartis, Sandoz, Christopher John Edwards Speakers bureau: Abbvie, Astra Zeneca, Celltrion, Chugai, Fresenius, Galapagos, Gilead, GSK, Lilly, Janssen, Pfizer, Roche, Consultant of: Abbvie, Astra Zeneca, Chugai, Galapagos, Gilead, GSK, Lilly, Janssen, Pfizer, Roche, Grant/research support from: Celltrion, Pfizer, Abbvie, Joao Eurico Fonseca Speakers bureau: Abbvie, Ache, Janssen, Lilly, Medac, Novartis, Pfizer, Consultant of: Abbvie, Celltrion, Janssen, Lilly, Pfizer, Grant/research support from: Abbvie, Janssen, Lilly, MSD, Novartis, Pfizer, Roche, Florenzo Iannone Speakers bureau: Abbvie, BMS, Celltrion, Galapagos, MSD, Eli-Lilly, Janssen, Novartis, Pfizer, UCB, Consultant of: Abbvie, BMS, Celltrion, Galapagos, MSD, Eli-Lilly, Janssen, Pfizer, Grant/research support from: BMS, MSD, Edward Keystone Speakers bureau: Amgen, AbbVie, Celltrion, F. Hoffmann-La Roche Inc., Janssen Inc., Merck, Pfizer Pharmaceuticals, Sandoz, Sanofi Genzyme, Consultant of: AbbVie, Amgen, Celltrion, Myriad Autoimmune, F. Hoffmann-La Roche Inc, Janssen Inc, Lilly Pharmaceuticals, Merck, Pfizer Pharmaceuticals, Sandoz, Sanofi-Genzyme, Samsung Bioepsis, Grant/research support from: Amgen, Merck, Pfizer Pharmaceuticals, Hendrik Schulze-Koops Consultant of: Celltrion, Taeksang Kwon Employee of: Celltrion Healthcare, Seungmin Kim Employee of: Celltrion Healthcare, Sangwook Yoon Employee of: Celltrion Healthcare, Dong-Hyeon Kim Employee of: Celltrion Healthcare, Gahee Park Employee of: Celltrion Inc., DaeHyun Yoo Speakers bureau: Celltrion, Celltrion Healthcare