fetching data ... 
Background: Rapidly progressive interstitial lung disease (RP-ILD) is often seen in dermatomyositis patients with anti-melanoma differentiation-associated gene 5 (anti-MDA-5) antibody. They often have a poor prognosis with rapid decline in pulmonary function, leading to respiratory failure (1). Aggressive immunosuppressive therapy has been reported with improved prognosis, however; it may lead to opportunistic infections, including cytomegalovirus (CMV) or Pneumocystis pneumonia (PCP) infection (2, 3).
Objectives: This study aimed to evaluate the effectiveness of tofacitinib (TOF) in combination with CMV and PCP prophylaxis in anti-MDA-5-positive patients.
Methods: Medical records of 17 anti-MDA-5-positive RP-ILD patients enrolled during Mar 2017 to May 2021 were reviewed. RP-ILD was defined by the presence of deteriorated dyspnea, with a decrease in PaO2 levels and emerging radiographic anomalies within 4 weeks without evidence of infection (4). Chest CT was scored using Ichikado score (5). Clinical parameters including ferritin levels, white counts (WBC), Lactate dehydrogenase (LDH) levels, GAP scores (Gender, Age, and Physiology score for idiopathic pulmonary fibrosis) were recorded. Medications included cyclophosphamide (CyP), intravenous immunoglobulin (IVIG), mycophenolic acid derivatives (MPA), rituximab (RTX), and calcineurin inhibitor (CNI). Kaplan-Meier survival analysis and Log-rank test were used to evaluate one-year mortality differences (MedCalc version 19.6). The Ethics Committee approved our study (CE17038B).
Results: Six anti-MDA-5-positive RP-ILD patients were treated with tofacitinib; five had concomitant CMV prophylaxis with valganciclovir (VGCV); 4 had PCP prophylaxis with trimethoprim/sulfamethoxazole (TMP-SMX). Patients’ demographic data are shown in
Clinical characteristics of anti-MDA-5 antibody-positive patients with RP-ILD receiving tofacitinib vs non-tofacitinib treatment.
| Tofacitinib (n=6) | Non-tofacitinib (n=11) | p value | |
|---|---|---|---|
| Age (years) | 58 (42.3-77) | 57 (50.0-62.0) | 0.884 |
| Female sex, n (%) | 2 (33.3) | 6 (54.5) | 0.620 |
| Diabetes mellitus, n (%) | 0 (0) | 5 (45.5) | 0.102 |
| Fever, n (%) | 5 (83.3) | 10 (90.9) | 1.000 |
| Mechanic’s hands, n (%) | 4 (66.7) | 5 (45.5) | 0.620 |
| Ferritin (n=16, ng/ml)) | 2670.9 (719.7-4209.7) | 1563.5 (967.8-3169.0) | 0.635 |
| WBC (x1000μl) | 8.7 (6.5-9.9) | 8.7 (6.0-12.9) | 0.884 |
| LDH (n=16, U/l) | 367.0 (218.0-557.5) | 433.0 (331.0-625.3) | 0.313 |
| GAP score | 5 (2.5-8) | 5 (2-6) | 0.808 |
| CT score | 200.0 (124.2-214.2) | 196.7 (153.3-273.3) | 0.733 |
| TMP-SMX, n (%) | 4 (66.7) | 0 (0) | 0.006** |
| VGCV, n (%) | 5 (83.3) | 0 (0) | 0.001** |
| CyP, n (%) | 1 (16.7) | 4 (36.4) | 0.600 |
| IVIG, n (%) | 1 (16.7) | 6 (54.5) | 0.304 |
| MPA, n (%) | 0 (0) | 7 (63.6) | 0.035* |
| RTX, n (%) | 3 (50.0) | 5 (45.5) | 1.000 |
| CNI, n (%) | 2 (33.3) | 6 (54.5) | 0.620 |
Continuous variables were expressed as median (inter-quartile range).
* p <0.05, ** p <0.01 by Mann–Whitney U test or Fisher’s Exact test.
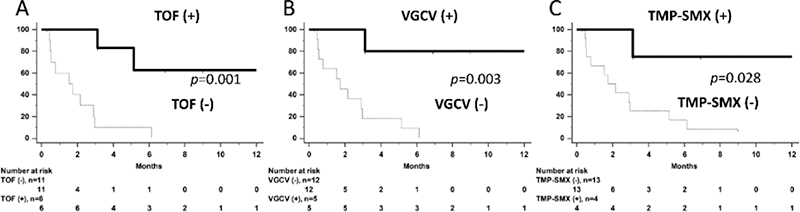
Conclusion: The study demonstrated the efficacy of tofacitinib treatment in anti-MDA-5-positive RP-ILD. In addition, CMV and PCP prophylaxis appeared to improve in 1-year survival. Rheumatologists might consider TOF with prophylaxis as an option for anti-MDA-5-positive patients in daily practice.
REFERENCES:
[1]Sato S, et al. Arthritis Rheum 2009;60(7):2193-200.
[2]Sekiguchi A, et al. J Dermatol 2020;47(8):876-81.
[3]Sabbagh SE, et al. Rheumatology 2021;60(2):829-36.
[4]Kurasawa K, et al. Rheumatology 2018;57(12):2114-19.
[5]Ichikado K, et al. Radiology 2006;238(1):321-9.
Acknowledgements: We are grateful to the Biostatistics Task Force staff of Taichung Veterans General Hospital for their assistance in performing the statistical analyses and Tomoko Hasegawa for her technical assistance with the immunoassays. We also thank Dr. Wen-Nan Huang, Dr. Pin-Kuei Fu, Dr. Chia-Wei Hsieh, Dr. Yi-Hsing Chen, and Dr. Der-Yuan Chen for their help on resources and supervision.
Disclosure of Interests: None declared