fetching data ... 
Background: There is a gap between how IIM patients are classified in practice and current validated classification criteria 1 . Also, different associations with genetic variations in HLA can inform about different T-cell mechanisms involved in disease pathogenesis.
Objectives: We aimed to systematically study associations between HLA-DRB1 alleles, clinical manifestations, and autoantibody-defined IIM subgroups.
Methods: We included 1348 IIM patients from five European countries. An unsupervised cluster analysis was performed using 14 autoantibodies: anti-Jo1, -PL7, -PL12, -EJ, -OJ, -SRP, -U1RNP, -Ro52, -Mi2, -TIF1γ, -MDA5, -PMScl, -SAE1, and -NXP2 to identify patients’ subgroups. Logistic regressions were used to estimate the associations between HLA-DRB1 alleles, clinical manifestations and the identified subgroups.
Results: Eight subgroups were defined by the autoantibody status (
Autoantibody-defined subgroups using an unsupervised cluster analysis.
| Subgroups/ Medoids | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | 1 Ro52 | 2 U1RNP | 3 PMScl | 4 Mi2 | 5 Jo1 | 6 Jo1/Ro52 | 7 TIF1 | 8 None* | All |
| n (% ) | 137 (10) | 183 (14) | 107 (8) | 65 (5) | 119 (9) | 140 (10) | 78 (6) | 519 (39) | 1348 (100) |
| Female (% ) | 93 (68) | 116 (63) | 79 (74) | 45 (69) | 76 (64) | 96 (69) | 64 (82) | 313 (60) | 882 (65) |
| Age at diagnosis, median (IQR) | 56 (16) | 51.5 (23) | 51 (25) | 57 (22.5) | 47.5 (23.25) | 52 (19.5) | 53.5 (21.75) | 58 (22) | 55 (23) |
| Autoantibodies | |||||||||
| Anti-Jo1 | 0 | 6 (3) | 0 | 1 (2) | 119 (100) | 140 (100) | 0 | 0 | 266 (20) |
| Anti-PL7 | 7 (5) | 13 (7) | 0 | 0 | 0 | 0 | 0 | 0 | 20 (1.5) |
| Anti-PL12 | 5 (4) | 3 (2) | 1 (1) | 0 | 1 (1) | 0 | 0 | 0 | 10 (0.7) |
| Anti-EJ | 2 (2) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 (0.1) |
| Anti-OJ | 0 | 7 (4) | 0 | 0 | 0 | 0 | 0 | 0 | 7 (0.5) |
| Anti-TIF1 | 10 (7) | 2 (1) | 2 (2) | 0 | 0 | 0 | 78 (100) | 0 | 92 (7) |
| Anti-Mi2 | 1 (1) | 1 (1) | 1 (1) | 65 (100) | 0 | 2 (1) | 0 | 0 | 70 (5) |
| Anti-SAE1 | 8 (6) | 23 (13) | 0 | 0 | 0 | 0 | 0 | 0 | 31 (2) |
| Anti-NXP2 | 1 (1) | 23 (13) | 1 (1) | 0 | 0 | 0 | 0 | 0 | 25 (2) |
| Anti-MDA5 | 9 (7) | 10 (6) | 1 (1) | 1 (2) | 0 | 1 (1) | 0 | 0 | 22 (2) |
| Anti-SRP | 8 (6) | 32 (18) | 0 | 0 | 0 | 0 | 0 | 0 | 40 (3) |
| Anti-Ro52 | 137 (100) | 16 (9) | 0 | 0 | 0 | 140 (100) | 0 | 0 | 293 (22) |
| Anti-PMScl | 11 (8) | 1 (1) | 107 (100) | 0 | 0 | 0 | 0 | 0 | 119 (9) |
| Anti-U1RNP | 0 | 79 (43) | 0 | 0 | 0 | 3 (2) | 0 | 0 | 82 (6) |
*IIM patients negative for the tested autoantibodies.
Forest plot of significant associations of HLA. *DRB1 alleles with autoantibody-defined subgroups. Scandinavia includes patients from Denmark, Norway, and Sweden.
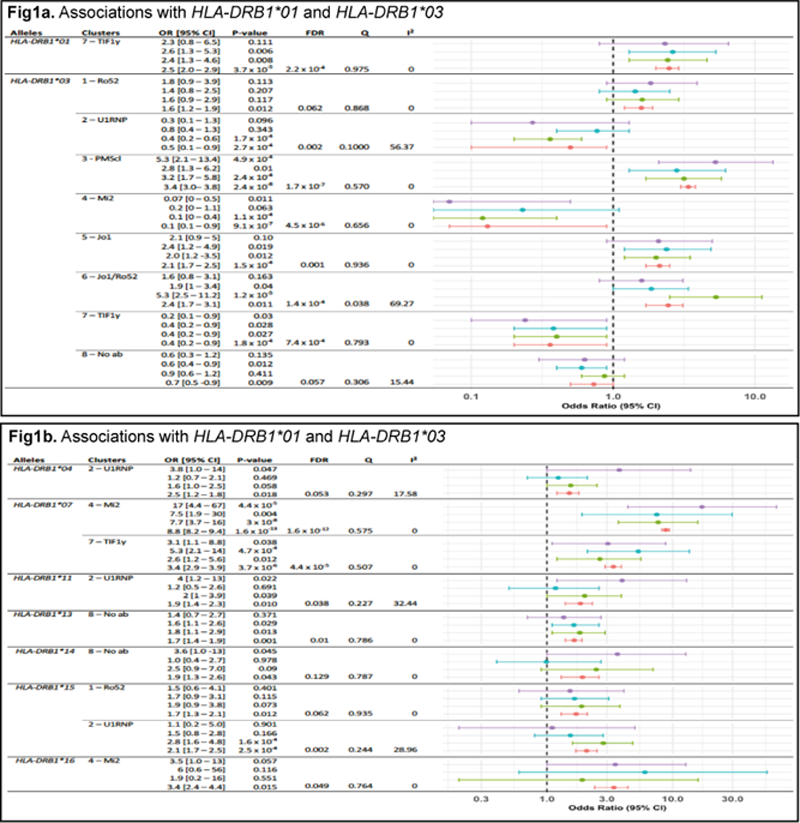
Conclusion: Our study reveals that certain subgroups of IIM patients are characterized by overlap of myositis -specific and -associated autoantibodies, which in turn are associated with different HLA-DRB1 alleles including potential novel associations. These results point to different disease mechanisms in the subgroups, as well as suggest that IIM classification could be improved by integrating broader serological and genetic data.
REFERENCES:
[1]Parker MJS, Oldroyd A, Roberts ME, et al. The performance of the European League Against Rheumatism/American College of Rheumatology idiopathic inflammatory myopathies classification criteria in an expert-defined 10 year incident cohort. Rheumatology (Oxford). 2019;58(3):468-475.
Acknowledgements: We thank all the patients who participated in the study.
Disclosure of Interests: Valerie Leclair: None declared, Angeles Shunashy Galindo-Feria: None declared, Simon Rothwell: None declared, Olga Kryštůfková: None declared, Heřman Mann: None declared, Louise Pyndt Diederichsen: None declared, helena andersson: None declared, Martin Klein: None declared, Sarah Tansley: None declared, Neil McHugh: None declared, Janine Lamb: None declared, Jiří Vencovský Speakers bureau: Abbvie, Biogen, Boehringer, Eli Lilly, Gilead, MSD, Novartis, Pfizer, Roche, Sanofi, UCB, Werfen, Consultant of: Abbvie, Argenx, Boehringer, Eli Lilly, Gilead, Octapharma, Pfizer, UCB, Grant/research support from: Abbvie, Hector Chinoy: None declared, Marie Holmqvist: None declared, Leonid Padyukov: None declared, Ingrid E. Lundberg Shareholder of: Roche and Novartis, Consultant of: Corbus Pharmaceuticals Inc, Astra Zeneca, Bristol Myer´s Squibb, Corbus Pharmaceutical, EMD Serono Research & Development Institute, Argenx, Octapharma, Kezaar, Orphazyme, and Janssen, Grant/research support from: Astra Zeneca, Lina M. Diaz-Gallo: None declared