fetching data ... 
Background: Management guidelines of RA suggest to administer biological or targeted synthetic DMARD (b/tsDMARD) in combination with conventional synthetic DMARD (csDMARD). Limited data exists about the impact of such csDMARD combination therapy (co-therapy) in real life settings, in particular for baricitinib use compared to other types of b/tsDMARD.
Objectives: To assess the impact of concomitant csDMARD prescription on b/tsDMARD maintenance, in a real-world setting.
Methods: This is a nested cohort study within the Swiss registry of RA patients (Swiss Clinical Quality Management (SCQM-RA)), of treatment courses with bDMARDs or baricitinib (BARI) initiated between 2017-09-01 and 2020-06-01, with at least one follow-up visit. We compared the time-to-drug-discontinuation (drug maintenance), as a measure of drug effectiveness of b/tsDMARDs, with or without csDMARD co-therapy. Our exposure of interest was the impact of csDMARD co-therapy compared to monotherapy in 3 categories of b/tsDMARDs: baricitinib (BARI), TNFi inhibitors (TNFi) and other modes of action bDMARDs (OMA). Co-therapy was defined as receiving at least one csDMARD during at least 40% of the b/tsDMARD treatment courses (TC) duration.
Baseline characteristics were compared using t-tests or χ 2 . Survival Kaplan-Meier curves, with Log-rank test, were used to assess time-to-discontinuation. Cox models were applied to obtain adjusted hazard ratios (HR) using age, BMI, corticosteroid treatment, CDAI score, disease duration, smoking, line of therapy, seropositivity, gender as covariates. Missing baseline CDAI values were imputed using linear model with quadratic regression time.
Results: 1065 TC were included (273 BARI, 319 OMA, 473 TNFi), about half of which were initiated with csDMARD co-therapy (
Baseline characteristics of studied population
| Variable | BARI | OMA | TNFi | ||||||
|---|---|---|---|---|---|---|---|---|---|
| BARI | BARI + csDMARD | p values | OMA | OMA + csDMARD | p values | TNFi | TNFi + csDMARD | p values | |
| n = 164 | n = 109 | n = 170 | n = 149 | n = 183 | n = 290 | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | |||||||
| Otherwise: % * | Otherwise: % * | Otherwise: % * | |||||||
| Prednisone | 21 % | 24 % | 0.73 | 22 % | 29 % | 0.18 | 20 % | 20 % | 1.00 |
| Line of Therapy | |||||||||
| - 1 st (= bio-naive) | 17 % | 18 % | 0.04 | 19 % | 22 % | 0.51 | 42 % | 51 % | 0.15 |
| -2 nd | 17 % | 24 % | 24 % | 22 % | 26 % | 20 % | |||
| -3 rd | 24 % | 11 % | 27 % | 20 % | 14 % | 10 % | |||
| -4 th or later | 42 % | 48 % | 31 % | 36 % | 19 % | 18 % | |||
| Female | 82 % | 73 % | 0.14 | 75 % | 71 % | 0.42 | 81 % | 70 % | 0.01 |
| Age | 60 (15) | 57 (11) | 0.05 | 60 (13) | 57 (12) | 0.03 | 52 (16) | 53 (14) | 0.66 |
| Disease duration (years ) | 13 (10) | 12 (9) | 0.82 | 11 (9) | 11 (10) | 0.58 | 9 (10) | 8 (8) | 0.36 |
| CDAI baseline | 19 (10) | 18 (8) | 0.53 | 20 (14) | 21 (12) | 0.53 | 18 (10) | 18 (11) | 0.64 |
| Seropositivity | 77 % | 72 % | 0.35 | 74 % | 75 % | 0.96 | 68 % | 71 % | 0.64 |
| csDMARD type | |||||||||
| - MTX | - | 48 % | - | - | 50 % | - | - | 60 % | - |
| - MTX + other | - | 2 % | - | 5 % | - | 4 % | - | ||
| - Other | - | 50 % | - | 45 % | - | 36 % | - | ||
TC = treatment course, BARI = baricitinib, TNFi = TNF inhibitors, OMA = Other Mode of Action drugs, DMARDs = Disease Modifying Anti-Rheumatic Drugs, csDMARDs = classical synthetic DMARDs, SD = standard deviation. CDAI = Clinical Disease Activity Index. csDMARD = conventional synthetic DMARD. MTX = Methotrexate. Other: Other csDMARD. * Percentages relate to total n treatment courses. p values in bold highlight statistically significant difference between respective groups. All % mean and SD values are rounded to integers.
Even after adjustment, we found no difference in drug maintenance with and without concomitant csDMARD in the BARI group (crude p = 0.67; HR co-therapy 2.17, 95% CI [0.61;7.77], p = 0.16) and in the TNFi group (crude p = 0.13; HR co-therapy 1.24, 95% CI [0.56;2.74], p = 0.60). Adjusted drug maintenance with or without csDMARD was also similar in the OMA group, despite non-adjusted p-value in favor of monotherapy (
Drug maintenance of monotherapy vs csDMARD co-therapy (Non-adjusted Kaplan-Meier).
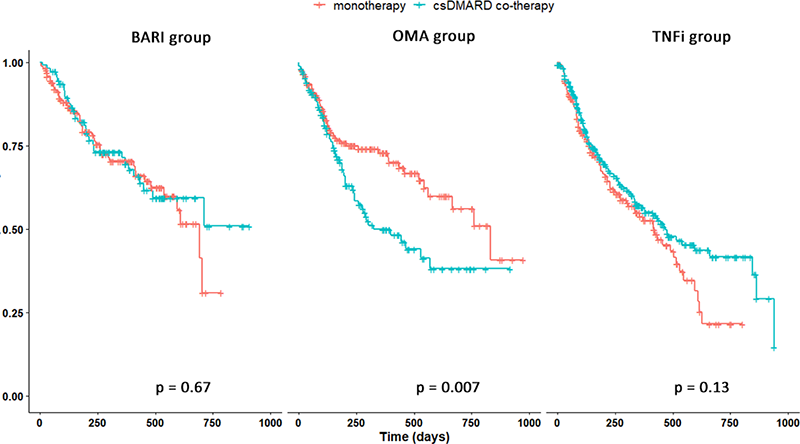
Conclusion: Our data suggest that drug maintenance of BARI, OMA and TNFi, were not significantly modified by concomitant csDMARD therapy.
Disclosure of Interests: Benoit GILBERT Speakers bureau: Once for Lilly, outside of the presented work., Denis Mongin: None declared, Eric Nham: None declared, Delphine Courvoisier: None declared, Kim Lauper Speakers bureau: for Pfizer, Viatris and Celltrion, outside of the submitted work., Consultant of: for Pfizer, outside of the submitted work., Cedric Laedermann Employee of: Currently employed by Eli Lilly., Rüdiger Müller: None declared, Axel Finckh Speakers bureau: Lilly, Grant/research support from: Research Grant by Lilly, to the rheumatology division.