fetching data ... 
Background: Upadacitinib (UPA) has demonstrated efficacy in patients with moderate-to-severe rheumatoid arthritis (RA) across various patient populations. 1–4
Objectives: This post hoc analysis aimed to evaluate the consistency in time to achieving meaningful clinical response with UPA 15 mg + conventional synthetic (cs) DMARDs in biologic (b) DMARD-inadequate responder (IR) versus csDMARD-IR patients with RA as well as with UPA 15 mg monotherapy versus UPA 15 mg + csDMARDs in csDMARD-IR patients.
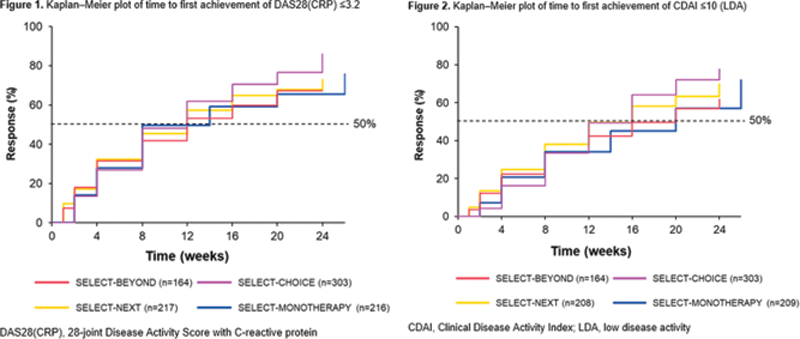
Methods: Patients originally randomized to UPA 15 mg once daily from four Phase 3 trials were included in this analysis: SELECT-BEYOND 1 and SELECT-CHOICE 2 (UPA 15 mg + csDMARDs in bDMARD-IR patients), SELECT-NEXT 3 (UPA 15 mg + csDMARDs in csDMARD-IR patients), and SELECT-MONOTHERAPY 4 (UPA 15 mg monotherapy in methotrexate-IR patients). Time to response was estimated using the Kaplan–Meier method for clinical outcomes over 24 weeks (26 weeks in SELECT-MONOTHERAPY). Clinical outcomes included achievement of 28-joint Disease Activity Score with C-reactive protein (DAS28[CRP]) ≤3.2; low disease activity (LDA) defined as Clinical Disease Activity Index (CDAI) ≤10 and Simple Disease Activity Index (SDAI) ≤11; and 50% improvement in American College of Rheumatology (ACR) core components and morning stiffness (MS) duration/severity. Data presented were as observed.
Results: Overall, 905 patients were included (SELECT-BEYOND: n=164; SELECT-CHOICE: n=303; SELECT-NEXT: n=221; SELECT-MONOTHERAPY: n=217). csDMARD-IR patients had a mean disease duration of 7.3 (SELECT-NEXT) or 7.5 years (SELECT-MONOTHERAPY); bDMARD-IR patients had a mean disease duration of 12.4 years, with a more refractory population (≥3 prior bDMARDs) in SELECT-BEYOND (23%) than SELECT-CHOICE (10%). In general, the median time to DAS28(CRP) ≤3.2, CDAI LDA, 50% improvement in ACR core components, and 50% improvement in MS duration/severity were consistent across the studies in bDMARD-IR and csDMARD-IR patients. For SELECT-BEYOND, SELECT-CHOICE, SELECT-NEXT, and SELECT-MONOTHERAPY, the median (95% CI) time to achieve DAS28(CRP) ≤3.2 was 12 (12, 16), 12 (8, 12), 12 (8, 12), and 14 (8, 14) weeks, respectively (
Conclusion: In diverse patient populations with RA, patients treated with UPA 15 mg, as monotherapy or with csDMARDs, generally demonstrated consistent time to achieving DAS28(CRP) ≤3.2, CDAI LDA, and 50% improvement in clinical outcomes.
REFERENCES:
[1]Genovese MC, et al. Lancet 2018;391:2513–24.
[2]Rubbert-Roth A, et al. N Engl J Med 2020;383:1511–21.
[3]Burmester GR, et al. Lancet 2018;391:2503–12.
[4]Smolen JS, et al. Lancet 2019;393:2303–11.
Acknowledgements: AbbVie funded this study; contributed to its design; participated in data collection, analysis, and interpretation of the data. No honoraria or payments were made for authorship. Medical writing support was provided by Amy Wilson, MSc, of 2 the Nth (Cheshire, UK), and was funded by AbbVie.
Disclosure of Interests: Andrea Rubbert-Roth Consultant of: AbbVie, Amgen, Bristol-Myers Squibb, Chugai, Eli Lilly, Gilead, Janssen, Novartis, Roche, and Sanofi, Bernard Combe Speakers bureau: AbbVie, Bristol-Myers Squibb, Celltrion, Eli Lilly, Gilead/Galapagos, Janssen, Merck, Novartis, Pfizer, Roche/Chugai, and Sanofi, Consultant of: AbbVie, Bristol-Myers Squibb, Celltrion, Eli Lilly, Gilead/Galapagos, Janssen, Merck, Novartis, Pfizer, Roche/Chugai, and Sanofi, Zoltán Szekanecz Speakers bureau: AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, Gedeon Richter, MSD, Pfizer, Roche, Sanofi, and UCB, Consultant of: AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, Gedeon Richter, MSD, Pfizer, Roche, Sanofi, and UCB, Stephen Hall Speakers bureau: Eli Lilly, Janssen, Merck, Novartis, Pfizer, and UCB; and research grants from AbbVie, Janssen, Merck, and UCB, Consultant of: Eli Lilly, Janssen, Merck, Novartis, Pfizer, and UCB; and research grants from AbbVie, Janssen, Merck, and UCB, Boulos Haraoui Speakers bureau: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, Merck, Novartis, Pfizer, and UCB, Consultant of: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, Merck, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Janssen, Merck, Novartis, Pfizer, and UCB, Suzan Attar: None declared, Anna-Karin H Ekwall Consultant of: AbbVie and Pfizer, Yanna Song Shareholder of: AbbVie Inc., Employee of: AbbVie Inc., Tim Shaw Shareholder of: AbbVie Inc., Employee of: AbbVie Inc., Orsolya Nagy Shareholder of: AbbVie Inc., Employee of: AbbVie Inc., Ricardo Xavier Consultant of: AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, Pfizer, and UCB