fetching data ... 
Background: Recent guidelines from the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) recommend that psoriatic arthritis (PsA) therapy achieve lowest possible disease activity across 6 key domains and related conditions. 1 In the DISCOVER-1&2 trials, guselkumab (GUS) significantly improved signs and symptoms of PsA at Week (W) 24.
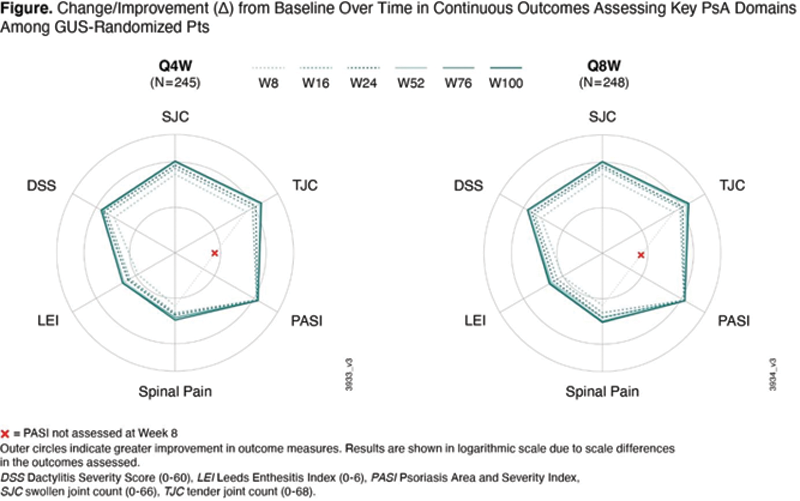
Objectives: Evaluate GUS efficacy through W100 of DISCOVER-2 by GRAPPA-recommended PsA domains (peripheral arthritis, skin, dactylitis, enthesitis, axial disease [nails not evaluated]) and related conditions of inflammatory bowel disease (IBD) and uveitis.
Methods: Enrolled adults had active PsA, were naïve to biologics/JAK inhibitors, and had ≥5 swollen and ≥5 tender joints and CRP ≥0.6 mg/dL. Randomized (1:1:1) patients (pts) received GUS 100 mg every 4 weeks (Q4W); GUS 100 mg at W0, W4, then every 8 weeks (Q8W); or placebo (PBO) with crossover to GUS 100 mg Q4W at W24. Outcomes selected aligned with GRAPPA-recommended domains/conditions: overall disease activity (Psoriatic Arthritis Disease Activity Score [PASDAS], Minimal Disease Activity [MDA]), peripheral arthritis (changes in Disease Activity Index for Psoriatic Arthritis [DAPSA] and clinical DAPSA [cDAPSA]), skin (Psoriasis Area and Severity Index [PASI], Investigator’s Global Assessment of psoriasis [IGA]), dactylitis (Dactylitis Severity Score [DSS]), enthesitis (Leeds Enthesitis Index [LEI]), axial disease (spinal pain) and IBD/uveitis (adverse events [AEs]). Among 493 GUS-randomized pts, change from baseline (BL) through W100 in continuous outcomes were analyzed by Repeated Measures Generalized Linear Mixed Effects Models adjusting for respective BL score and GUS regimen. Achievement of therapeutic endpoints was summarized by descriptive statistics using nonresponder imputation (NRI) for missing categorical data.
Results: ~90% of GUS-randomized pts completed treatment at W100. For continuous outcomes, improvements over time in key PsA domains extended through W100 of GUS (
Number (%) of GUS-randomized Pts (N=493) Achieving Therapeutic Endpoints Over Time (NRI ) *
| Week | Q4W | Q8W | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 8 | 16 | 24 | 52 | 100 | 8 | 16 | 24 | 52 | 100 | |
| MDA * | 8 (3) | 33 (14) | 47 (19) | 83 (34) | 93 (38) | 9 (4) | 42 (17) | 63 (25) | 77 (31) | 100 (40) |
| DAPSA | 43 (18) | 61 (25) | 88 (36) | 125 (51) | 151 (62) | 43 (17) | 79 (32) | 97 (39) | 130 (52) | 147 (59) |
| ≤14’; | ||||||||||
| ≤4 | 5 (2) | 12 (5) | 21 (9) | 39 (16) | 52 (21) | 3 (1) | 15 (6) | 23 (9) | 46 (19) | 60 (24) |
| cDAPSA | 41 (17) | 58 (24) | 89 (36) | 125 (51) | 150 (61) | 44 (18) | 75 (30) | 95 (38) | 131 (53) | 147 (60) |
| ≤13 * | ||||||||||
| ≤3 | 5 (2) | 13 (5) | 29 (12) | 44 (18) | 59 (24) | 4 (2) | 19 (8) | 25 (10) | 53 (21) | 65 (26) |
| PASDAS | ||||||||||
| ≤3.2 | 25 (10) | 44 (18) | 58 (24) | 105 (43) | 126 (51) | 28 (11) | 56 (23) | 76 (31) | 106 (43) | 122 (49) |
| ≤1.9 | 4 (2) | 11 (4) | 22 (9) | 36 (15) | 51 (21) | 2 (1) | 16 (6) | 23 (9) | 52 (21) | 58 (23) |
| Skin | ||||||||||
| PASI75 † | - | 137 (74) | 146 (79) | 160 (87) | 152 (83) | - | 129 (73) | 139 (79) | 151 (86) | 144 (82) |
| PASI90 † | - | 100 (54) | 114 (62) | 142 (77) | 136 (74) | - | 97 (55) | 121 (69) | 131 (74) | 123 (70) |
| PASI100 † | - | 62 (34) | 83 (45) | 106 (58) | 109 (59) | - | 48 (27) | 80 (46) | 93 (53) | 94 (53) |
| IGA 0/1 Response ‡ | - | 122 (66) | 127 (69) | 147 (80) | 140 (76) | - | 110 (62) | 124 (70) | 131 (74) | 126 (72) |
| Enthesitis resolution § | 45 (27) | 66 (40) | 71 (43) | 93 (56) | 102 (61) | 50 (32) | 75 (48) | 87 (55) | 97 (62) | 110 (70) |
| Dactylitis resolution § | 39 (32) | 64 (53) | 80 (66) | 90 (74) | 87 (72) | 34 (31) | 51 (46) | 66 (60) | 86 (77) | 92 (83) |
* Repeated Measures Generalized Linear Mixed Effects Models; excludes pts who achieved endpoint at BL.
† Pts with BL IGA≥2 and BSA≥3%.
‡ IGA skin response = score of 0 or 1 and ≥2 grade improvement from BL.
§ Among pts with domain at BL.
Conclusion: In DISCOVER-2 bio-naïve PsA pts, both GUS regimens provided continued improvements in key GRAPPA-recommended domains of PsA through up to 2 years of treatment.
REFERENCES:
[1]Coates et al. Ann Rheum Dis 2021;80(suppl 1):139
Disclosure of Interests: Laura Coates Speakers bureau: AbbVie, Amgen, Biogen, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, Medac, Novartis, Pfizer and UCB, Consultant of: AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Gilead, Galapagos, Janssen, Novartis, Pfizer, and UCB, Grant/research support from: AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, and UCB, Laure Gossec Consultant of: AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead, GSK, Janssen, Novartis, Pfizer, Samsung Bioepis, Sanofi-Aventis, and UCB, Grant/research support from: Amgen, Eli Lilly, Galapagos, Pfizer, and Sandoz, Christine CONTRE Shareholder of: Johnson & Johnson, Employee of: Janssen Cilag, May Shawi Shareholder of: Johnson & Johnson, Employee of: Janssen Pharmaceutical Companies of Johnson & Johnson, Emmanouil Rampakakis Consultant of: Janssen, Employee of: JSS Medical Research, Natalie Shiff Shareholder of: Johnson & Johnson, Employee of: Janssen Scientific Affairs, LLC, Alexa Kollmeier Shareholder of: Johnson & Johnson, Employee of: Janssen Research & Development, LLC, Xie L Xu Shareholder of: Johnson & Johnson, Employee of: Janssen Research & Development, LLC, Peter Nash Grant/research support from: Janssen, Abbvie, Pfizer, Novartis, Lilly, Gilead, Roche, Sandoz, Celgene, Sun, Boehringer, and Bristol Myers Squibb, Philip J Mease Speakers bureau: AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer, Sun Pharma, and UCB, Consultant of: AbbVie, Aclaris, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead, GSK, Inmagene, Janssen, Novartis, Pfizer, Sun Pharma, and UCB, Grant/research support from: AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer, Sun Pharma, and UCB, Philip Helliwell Paid instructor for: Abbvie, Amgen, Novartis, Janssen, Consultant of: Eli Lilly