fetching data ... 
Background: Drug maintenance is a common outcome measure of real world effectiveness studies, because it combines a measure of drug effectiveness and its tolerance / safety. Major hurdles of observational studies are potential selection biases and confounding. Cox proportional hazard ratio models address this issue by adjusting for potential confounders, but misspecification of the model may lead to biased estimates. ‘Augmented Inverse Probability Treatment Weighting’ (AIPTW) has the attractive property of being doubly robust, meaning that only one of the two underlying models has to be correctly specified to obtain consistent estimates. It can be used as a sensitivity analysis for Cox models, when analyzing time-to-event data.
Objectives: To evaluate AIPTW estimator and test the robustness of the results obtained by a Cox model.
Methods: Previous analyses in the Swiss rheumatoid arthritis (RA) registry (SCQM) had demonstrated that time to all-cause-discontinuation was significantly longer in RA patients on bariticinib (BARI, N = 273) compared to TNF-inhibitors (TNFi, N = 473); but not compared to other mode of actions biologics (OMA, N = 378) [1], in an adjusted Cox regression including age, gender, BMI, concomitant csDMARD, prednisone, CDAI score, disease duration, smoking status, line of therapy and seropositivity.
Here we repeat the same analysis using AIPTW, including the same potential confounders. We combine a propensity score using a logistic regression model and an inverse probability weighted Cox regression. Two implementations of the AIPTW estimator are considered. First we use the RiskRegression package in R, to obtain risk ratios. Then we implement the AIPTW manually to obtain the average treatment effect as the difference in median survival time.
Results: Time to treatment discontinuation measured with Cox model was significantly longer for RA patients on BARI compared to patients on TNFi according to the adjusted Cox model (HR = 1.79), and a similar non-significant trend existed when compared to OMA (HR = 1.29).
When considering 90-day treatment discontinuation measured with the AIPTW, the results were qualitatively very similar: the risk ratio between BARI and TNFi groups is statistically significant (RR = 2.51), while that of BARI against OMA is larger than one (RR = 1.47), but not statistically significant. Confidence intervals are larger with the AIPTW estimation.
Cox Regression HR and AIPTW risk ratios
| Cox Regression Hazard Ratio (95% CI) | AIPTW Estimate of 90-day risk ratio of treatment discontinuation (95% CI) | |
|---|---|---|
| BARI vs. TNFi | 1.79* (1.34-2.38) | 2.51* (1.19 – 3.83) |
| BARI vs. OMA | 1.29 (0.96-1.73) | 1.47 (0.76 – 2.18) |
Legend: BARI: baricitinib; TNFi: TNF-inhibitors; OMA: Other Mode of Actions biologics; AIPTW: Augmented Inverse Probability Treatment Weighting. 95% CI: 95% Confidence Interval. *: statistically significant result at the p<0.05 level.
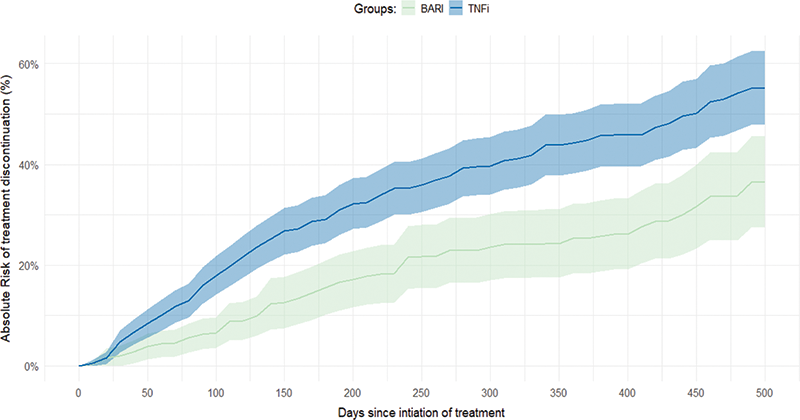
Absolute risk of treatment discontinuation over time between patients on baricitinib and patients on TNF inhibitors, estimated with AIPTW.
Conclusion: Time to treatment discontinuation measured with Cox model was significantly longer for RA patients on BARI compared to patients on TNFi according to the adjusted Cox model (HR = 1.79), and a similar non-significant trend existed when compared to OMA (HR = 1.29).
When considering 90-day treatment discontinuation measured with the AIPTW, the results were qualitatively very similar: the risk ratio between BARI and TNFi groups is statistically significant (RR = 2.51), while that of BARI against OMA is larger than one (RR = 1.47), but not statistically significant. Confidence intervals are larger with the AIPTW estimation.
Conflict of Interest: This analysis has been made possible by financial support of Eli Lilly (Suisse) SA to the Geneva University Hospitals (HUG).
REFERENCES:
[1]Ann Rheum Dis, supplement 1, year 2021. DOI: 10.1136/annrheumdis-2021-eular.1781
Disclosure of Interests: Romain Aymon: None declared, Benoit GILBERT: None declared, Denis Mongin: None declared, Eric Nham: None declared, Cedric Laedermann Employee of: Eli Lilly, Rüdiger Müller Consultant of: Streuli Pharma, Gebro Pharma, AbbVie, Kim Lauper Speakers bureau: Pfizer, Viatris and Celltrion, Consultant of: Pfizer, Delphine Courvoisier: None declared, Axel Finckh: None declared