fetching data ... 
Background A rise in the incidence of selected autoimmune disorders has been described, raising the question as to whether the overall incidence of autoimmune disorders might be on the rise due to environmental factors. However, reliable estimates of disease incidence and trends over time, particularly as pertains to autoimmune diseases as a group, are not available. Commonalities and differences between individual diseases also remain poorly understood.
Objectives To investigate the incidence and prevalence for 19 of the most common autoimmune diseases, to assess trends over time, by sex, age, socioeconomic status, season and region, and to examine rates of co-occurrence among autoimmune diseases.
Methods We used linked primary and secondary electronic health records of 22 million individuals from the Clinical Practice Research Datalink (CPRD), a cohort that is representative of the UK population in terms of age and sex. We calculated incidence and prevalence of 19 autoimmune disorders from 2000 to 2019 and used negative binomial regression models to investigate temporal trends and variation by age, sex, socioeconomic status, season of onset and region. To characterise co-occurrence of autoimmune diseases, we calculated incidence rate ratios, comparing incidence rates of comorbid autoimmune disease among patients with a first autoimmune disease with incidence rates in the general population, using negative binomial regression models, adjusted for age and sex.
Results Among the 22,009,375 individuals included in the study, we identified a total of 978 872patients with a new diagnosis of at least one autoimmune disease between 2000 and 2019 (mean (SD) age: 54.0 (21.4) years, 64% women). Over the study period, age-standardised incidence rates of autoimmune diseases increased by 4%, similarly for men and women. The largest increases were seen in Graves’ disease, coeliac disease and Sjogren’s syndrome, for which incidences have doubled over the past two decades. Two conditions exhibited a significant decrease in incidence (Hashimoto’s thyroiditis and pernicious anaemia). Taken together the 19 autoimmune disorders examined affected 10.2% of the population over the study period (13.1% of women, 7.4% of men). A socioeconomic gradient was evident across several diseases, including Graves’ disease, pernicious anaemia, rheumatoid arthritis, and systemic lupus erythematosus. Seasonal variations were observed for type 1 diabetes (more commonly diagnosed in winter) and vitiligo (more commonly diagnosed in summer), and regional variations were observed for a range of conditions. Autoimmune disorders were commonly associated with each other, particularly Sjogren’s, systemic lupus erythematosus and systemic sclerosis. Patients with type 1 diabetes also had significantly higher rates of Addison’s, coeliac, and thyroid diseases, and multiple sclerosis stood out as having low rates of co-occurrence with other autoimmune diseases.
Conclusion Autoimmune diseases affect about one in ten individuals. Their burden continues to increase over time, albeit at varying rates across individual diseases. The socioeconomic, seasonal, and regional disparities observed among several autoimmune disorders, implicate environmental factors in disease pathogenesis. The interrelations between autoimmune diseases are commensurate with shared pathogenetic mechanisms or predisposing factors, particularly among connective tissue diseases and among endocrine diseases.
Image/graph:
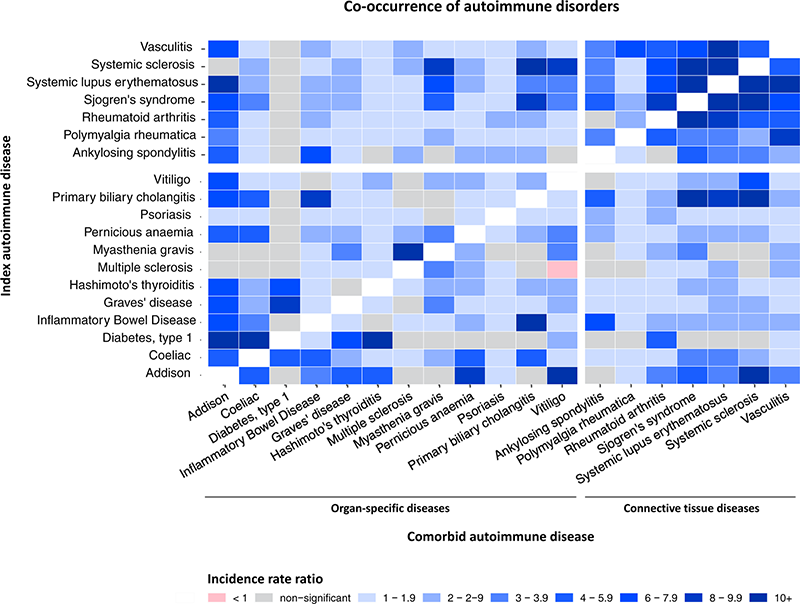
Figure 1. Incidence rate ratios for development of comorbid autoimmune disease among index populations with autoimmune disease compared with the general population
Incidence rate ratios were calculated for development of a second (comorbid) autoimmune disease among index populations with pre-existing autoimmune disease compared with the general population using negative binomial regression models adjusted for age and sex. Diabetes refers to childhood-onset type 1 diabetes (people aged <20 years at diagnosis).
Acknowledgements This project has received funding from the Research Foundation Flanders (grant number 12ZU922N).
Disclosure of Interests Nathalie Conrad: None declared, Shivani Misra: None declared, Jan Verbakel: None declared, Geert Verbeke: None declared, Geert Molenberghs: None declared, Peter Taylor: None declared, Justin Mason: None declared, Naveed Sattar Speakers bureau: NS declares consulting fees and/or speaker honoraria from Abbott Laboratories, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, and Sanofi; and grant support paid to his university from AstraZeneca, Boehringer Ingelheim, Novartis, and Roche Diagnostics., Consultant of: NS declares consulting fees and/or speaker honoraria from Abbott Laboratories, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, and Sanofi; and grant support paid to his university from AstraZeneca, Boehringer Ingelheim, Novartis, and Roche Diagnostics., John McMurray Speakers bureau: JJVM has received funding to his institution from Amgen and Cytokinetics for his participation in the Steering Committee for the ATOMIC-HF, COSMIC-HF, and GALACTIC-HF trials and meetings and other activities related to these trials; has received payments through Glasgow University from work on clinical trials, consulting and other activities from Alnylam, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cardurion, Dal-Cor, GlaxoSmithKline, Ionis, KBP Biosciences, Novartis, Pfizer, and Theracos; has received personal lecture fees from the Corpus, Abbott, Hikma, Sun Pharmaceuticals, Medscape/Heart.Org, Radcliffe Cardiology, Servier Director, and Global Clinical Trial Partners (GCTP)., Consultant of: JJVM has received funding to his institution from Amgen and Cytokinetics for his participation in the Steering Committee for the ATOMIC-HF, COSMIC-HF, and GALACTIC-HF trials and meetings and other activities related to these trials; has received payments through Glasgow University from work on clinical trials, consulting and other activities from Alnylam, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cardurion, Dal-Cor, GlaxoSmithKline, Ionis, KBP Biosciences, Novartis, Pfizer, and Theracos; has received personal lecture fees from the Corpus, Abbott, Hikma, Sun Pharmaceuticals, Medscape/Heart.Org, Radcliffe Cardiology, Servier Director, and Global Clinical Trial Partners (GCTP)., Iain McInnes Speakers bureau: IM declares honoraria from AbbVie; grant support paid to his university from AstraZeneca and Eli Lilly; participation on data safety monitoring boards/advisory boards of AstraZeneca, BMS, Eli Lilly, Novartis, Janssen, GSK, AbbVie, Cabaletta, Compugen, Causeway, Gilead, Moonlake, Reflexion, UCB, XinThera; patents from Novartis; leadership roles with Evelo, Versus Arthritis, and Greater Glasgow and Clyde Health Board; and stock or stock options with Evelo, Compugen, and Cabaletta., Consultant of: IM declares honoraria from AbbVie; grant support paid to his university from AstraZeneca and Eli Lilly; participation on data safety monitoring boards/advisory boards of AstraZeneca, BMS, Eli Lilly, Novartis, Janssen, GSK, AbbVie, Cabaletta, Compugen, Causeway, Gilead, Moonlake, Reflexion, UCB, XinThera; patents from Novartis; leadership roles with Evelo, Versus Arthritis, and Greater Glasgow and Clyde Health Board; and stock or stock options with Evelo, Compugen, and Cabaletta., Kamlesh Khunti Speakers bureau: KK has also acted as a consultant, speaker or received grants for investigator-initiated studies for Astra Zeneca, Bayer, Novartis, Novo Nordisk, Sanofi-Aventis, Lilly and Merck Sharp & Dohme, Boehringer Ingelheim, Oramed Pharmaceuticals and Applied Therapeutics., Consultant of: KK has also acted as a consultant, speaker or received grants for investigator-initiated studies for Astra Zeneca, Bayer, Novartis, Novo Nordisk, Sanofi-Aventis, Lilly and Merck Sharp & Dohme, Boehringer Ingelheim, Oramed Pharmaceuticals and Applied Therapeutics., Grant/research support from: KK has also acted as a consultant, speaker or received grants for investigator-initiated studies for Astra Zeneca, Bayer, Novartis, Novo Nordisk, Sanofi-Aventis, Lilly and Merck Sharp & Dohme, Boehringer Ingelheim, Oramed Pharmaceuticals and Applied Therapeutics., Geraldine Cambridge: None declared.
Keywords: Real-world evidence, Gender/diversity issues, Epidemiology
DOI: 10.1136/annrheumdis-2023-eular.4269