fetching data ... 
Background Infections are a major cause of morbidity and mortality in juvenile systemic lupus erythematosus (SLE).
Objectives We assessed the incidence and risk factors for major infections in juvenile SLE.
Methods A retrospective review of 225 patients of juvenile SLE (ACR 1997 criteria) with age <18 years visiting the rheumatology clinic at a single centre between 2000 to 2020 was done from clinical case records and data from the hospital electronic health records. Serious infection was defined as the need for hospitalization, or infection resulting in disability or death. Cox regression was used to determine factors associated with a serious infection and the effect of serious infection on overall survival.
Results Among the 225 children (197 girls) with a mean age of 13.89 ±3.42 years and a cumulative follow up of 1153.45 person-years. A total of 80 serious infections occurred in 63 (28% of the cohort) individuals at a rate of 69.35 serious infections per 1000 person-years of follow-up. A second serious infection occurred in 12 children and 5 of them developed a third serious infection. Among the microbiologically confirmed cases (78.75% of cases) Bacterial infections were most common (N=33) and included S. Aureus (11), E. Coli (7), K. Pneumoniae (3), E. Fecalis (3), S. Pneumoniae (2), Acinetobacter spp. (2), Citrobacter (2), Salmonella (2) and P. Aeruginosa [1]. Twenty six (32.5%) opportunistic infections occurred: Mycobacterium tuberculosis (18), Cytomegalovirus (3), disseminated Herpes zoster (4) and invasive candidiasis (1) with 15 (83.3%) of the tuberculosis cases being extrapulmonary. On multivariate analysis fever at baseline(HR 8.51, 1.17-61.44), gastrointestinal involvement (HR 4.73, 1.13-19.94), current steroid dose (HR 1.36,1.14-1.62), average cumulative steroid dose per year (HR 1.004, 1.002-1.005) and cyclophosphamide use (HR 2.22, 1.11-4.46) were associated with serious infection (Table 1). Hospitalization rates were significantly higher in those with any serious infection (Rate ratio 2.79, 1.81-3.77). Serious infection led to more damage accrual (SLICC damage index 1.04 vs 0.22). Serious infection-free survival at 1 year, 5 years and 10 years was 84% (79.1-89.2) and 72% (65.4-79.2). There were 19 deaths with infection attributable mortality in 10 (52.6%). Serious infection predisposed to higher overall mortality (Figure 1).
Conclusion Serious infections are a major cause of mortality and damage accrual in SLE. Constitutional symptoms, gastrointestinal involvement, current and cumulative steroid dose and cyclophosphamide use predict serious infections. TB prophylaxis in patients with SLE should be considered in endemic areas, especially when using high-dose steroid therapy.
| Covariates | Hazard ratio | 95% CI |
|---|---|---|
| Fever* | 8.51 | 1.17-61.45 |
| Serositis | 0.81 | 0.41-1.59 |
| Gastrointestinal involvement* | 4.76 | 1.94-19.94 |
| Major organ manifestation | 1.07 | 0.49-2.31 |
| SLEDAI-2K | 0.99 | 0.95-1.05 |
| Daily steroid dose (/10mg)* | 1.36 | 1.14-1.62 |
| Mean cumulative steroid dose* | 1.004 | 1.002-1.005 |
| Albumin | 1.01 | 0.66-1.55 |
| Absolute lymphocyte count | 0.99 | 0.99-1 |
| Cyclophosphamide use* | 2.22 | 1.11-4.46 |
*-significant baseline predictors of serious infection on follow up. Major organ manifestation referes to presence of nephritis or neuropsychiatric lupus.
Image/graph:
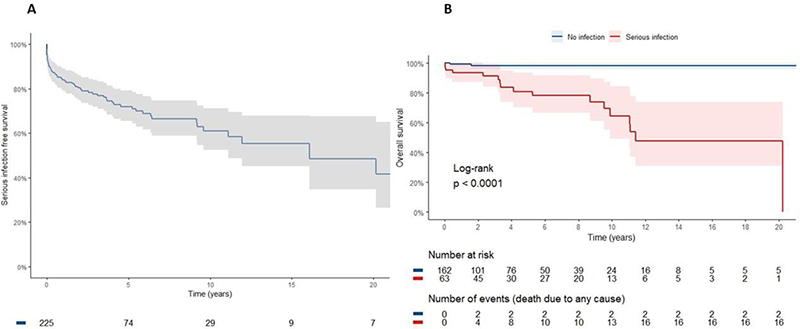
Figure 1. A. The Kaplan meier survival curve depicts time to first serious infection. B. The Kaplan meier survival curve shows the overall survival difference between those with any serious infection ever compared to those with no serious infection in the disease course.
REFERENCES:
NIL.
Acknowledgements: NIL.
Disclosure of Interests None Declared.
Keywords: Prognostic factors, Systemic lupus erythematosus
DOI: 10.1136/annrheumdis-2023-eular.5338