fetching data ... 
Background Hydroxychloroquine (HCQ) is a widely used drug in Systemic Lupus Erythematosus (SLE) that can cause cardiac alterations such as arrhythmic events in the short-term and dose-dependent cardiomyopathy in the medium to long-term. The cardiological implications of HCQ accumulation in these patients in the medium to long-term is unknown.
Objectives To assess the optimal cut-off point for electrocardiogram (ECG) in patients with SLE on HCQ therapy to prevent arrhythmic complications.
Methods Single university hospital observational study of all consecutive SLE patients who had an ECG at baseline and at least one ECG at follow-up. New conduction disturbances were assessed by ECG, defined as atrioventricular block, bundle branch block or QT interval prolongation. ECGs were extracted from the medical record and interpreted at baseline and for 15.2 years (95%CI 13.24-17.16) of follow-up. We defined cumulative HCQ (cHCQ) as the total grams of HCQ that had been administered. A Receiver Operating Characteristic (ROC) curve analysis was performed to determine the optimal cut-off point for sensitivity and specificity.
Results We studied 105 (93 female/12 male) SLE patients with a mean (±SD) age of 61.8±14.9 years. The mean daily dose of HCQ in our sample was 256 mg per day (Table 1). The ROC curve showed a moderate diagnostic ability for new conduction disturbances with an area under the curve of 0.69 (95% CI 0.59 - 0.77) (Figure 1). The highest efficacy cut-off point was cHCQ: 4097g (Sensitivity 15%; Specificity 100%) and the optimal cut-off point was cHCQ: 901g (Sensitivity 85%; Specificity 52.9%). This cut-off point was reached with a mean HCQ treatment in our sample of 9.7 years. High grade atrio-ventricular block was found in 5 patients. In all of them the cHCQ dose was over 901g.
Conclusion According to our study, 901g of cHCQ dose is a good cut-off point for performing a protocolized ECG to rule out cardiac conduction disturbances in patients with SLE and chronic HCQ treatment. This is equivalent to 9.7 years of treatment with the mean HCQ dose use in our sample.
| General characteristics | Global (N=105) |
|---|---|
| Current age (mean ± SD) | 61.8 ± 14.9 |
| Years of SLE evolution (mean ± SD) | 16.3 ± 10.3 |
| Sex, n (%) | 93 (88.6) |
| Diabetes Mellitus, n (%) | 15 (14.4) |
| Hypertension, n (%) | 58 (55.2) |
| Dyslipidaemia, n (%) | 47 (45.2) |
| Chronic renal failure, n (%) | 10 (9.6) |
| Obesity, n (%) | 8 (7.8) |
| Alcohol consumption, n (%) | 3 (2.9) |
| Smoking history, n (%) | 41 (39.0) |
| SLE treatment | |
| HCQ dose in mg/day (mean ± SD) | 256 ± 87.2 |
| Time in HCQ in months (mean ± SD) | 149.8 ± 111.9 |
| Cumulative HCQ dose in grams (mean ± SD) | 1154.94 ± 946.10 |
| Cumulative HCQ dose in grams, median (IQR) | 913.1 (474, 1473) |
| Prednisone, n (%) | 30 (28.6) |
| Prednisone dose in mg/day (mean ± SD) | 17.3 ± 16.8 |
| Other immunosuppressant, n (%) | 14 (13.3) |
Abbreviations: HCQ: Hydroxychloroquine, SLE: Systemic Lupus Erythematosus
Image/graph:
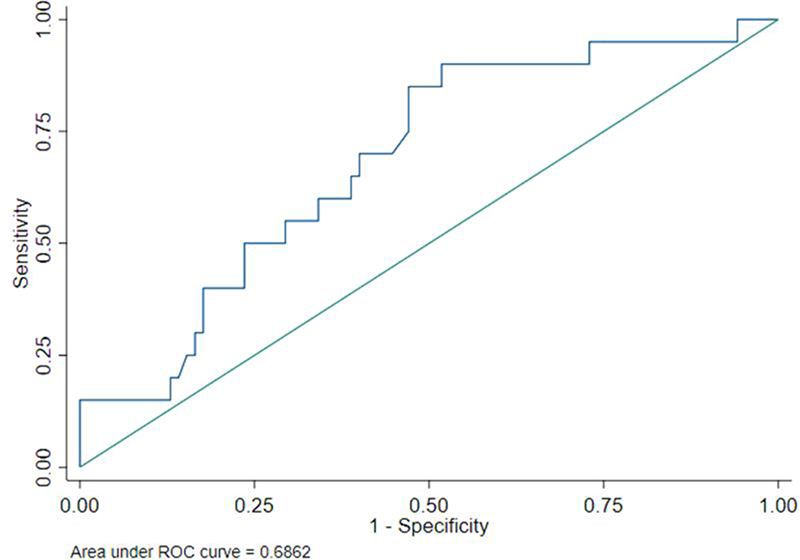
Figure 1. Receiver Operating Characteristic (ROC) curve on cumulative hydroxychloroquine dose and new conduction disturbances
REFERENCES:
NIL.
Acknowledgements: NIL.
Disclosure of Interests Alba Herrero-Morant: None declared, Jon Zubiaur-Zamacola: None declared, Adrián Margarida-de Castro: None declared, Raquel Pérez-Barquín: None declared, Ricardo Blanco Speakers bureau: Abbvie, Pfizer, Roche, Lilly, Bristol-Myers, Janssen, Galapagos and MSD, Consultant of: Abbvie, Pfizer, Roche, Lilly, Bristol-Myers, Janssen and MSD, Grant/research support from: Abbvie, MSD, Novartis and Roche.
Keywords: Disease-modifying drug (DMARDs), Systemic lupus erythematosus
DOI: 10.1136/annrheumdis-2023-eular.4462