fetching data ... 
Background The pathophysiology of Systemic Lupus Erythematosus (SLE) involves genetic and acquired immune dysregulation, both of which predispose patients to infection. Infections are a leading cause of hospital admission, intensive care unit admission and death.
Objectives To evaluate the frequency and associated factors of hospitalizations due to infections in patients with SLE.
Methods Cross-sectional study carried out with the RELESSAR trans registry. Patients with SLE (ACR 1997 criteria) were included. Sociodemographic variables, autoantibodies, manifestations of the disease, comorbidities and activity and chronicity index were analyzed. A serious infection was defined as one that required hospitalization. We evaluated number and localization of the infections, microorganisms and treatments received during the admissions and these variables were compared between patients hospitalized versus not hospitalized.
Results A total of 1515 patients participated in the registry and 815 patients had been admitted: 41 cases were hospitalized due to infection exclusively and 162 patients of both infection and flare of the disease (total=203).
The mean time of admissions was 1.42 (SD 0.99). Graphic 1 shows the number of serious infections per patient. The most frequent localization was the respiratory tract and bacterial were the most frequently microorganism isolated. We compared 203 patients and 646 patients not hospitalized (Table 1).
In multivariate analysis, age at SLE diagnosis (OR 0.96 95%CI 0.94-0.98, p< 0.001), level of education (OR 0.89 95%CI 0.83-0.94, p< 0.001), pericarditis (OR 3.25 95%CI 1.89-5.60, p< 0.001), low complement (OR 3.16 95%CI 1.33-8.10, p=0.010), SLICC index (OR 1.95 95%CI 1.61-2.37, p< 0.001) and 10-30 mg/d of prednisone (OR 3.70 95%CI 1.66-9.00, p=0.002), 30-60 mg/day of prednisone (OR 8.40 95%CI 3.58-21.5, p< 0.001), azathioprine (OR 1.67 95%CI 1.02-2.73, p= 0.042), mycophenolate (OR 2.15 95%CI 1.27-3.67, p=0.005) and Igiv (OR 8.25 95%CI 2.33-39.3, p=0.003) were variables independently associated to hospitalization due to infection.
Image/graph:
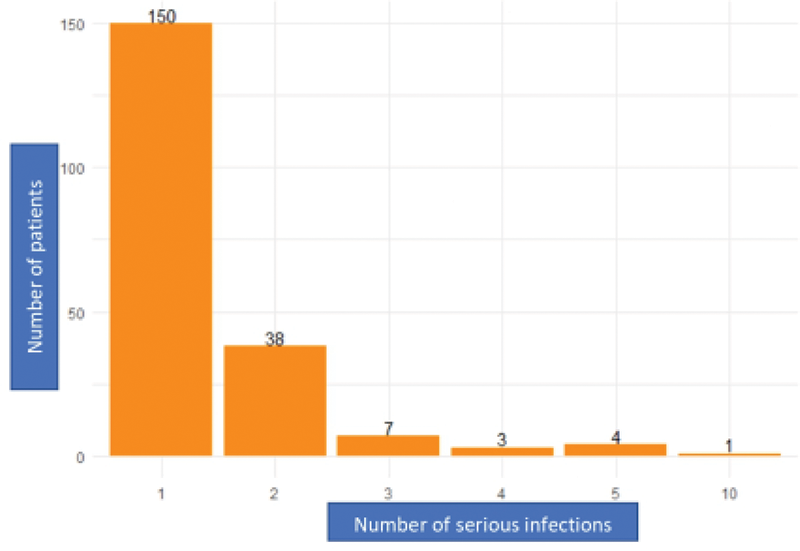
Graphic 1. Number of serious infections per patient.
| Hospitalization due to infection |
Non hospitalization |
Total |
P-value | |
|---|---|---|---|---|
| Age at SLE diagnosis |
25.4 [18.9, 34.6] | 30.6 [23.0, 40.7] | 29.1 [21.9, 39.2] | <0.001 |
| Years of education |
10.9 (3.76) | 12.7 (3.95) | 12.3 (3.98) | <0.001 |
| Pericarditis | 76 (37.6%) | 68 (10.6%) | 144 (17.1%) | <0.001 |
| Lupus Nephritis | 121 (59.6%) | 160 (25.0%) | 281 (33.3%) | <0.001 |
| Convulsion | 23 (11.3%) | 22 (3.45%) | 45 (5.36%) | <0.001 |
| Anti-DNA | 160 (78.8%) | 370 (58.4%) | 530 (63.3%) | <0.001 |
| Low complement | 136 (68.0%) | 333 (53.7%) | 469 (57.2%) | <0.001 |
| Charlson index |
2.00 [1.00, 3.00] | 1.00 [1.00, 3.00] | 1.00 [1.00, 3.00] | <0.001 |
| SLICC index |
1.00 [1.00, 3.00] | 0 [0, 1.00] | 1.00 [0, 1.00] | <0.001 |
| SLEDAI Median [Q1, Q3] | 2.00 [0, 5.00] | 2.00 [0, 4.00] | 2.00 [0, 4.00] | 0.073 |
| 10-30 mg/day | 89 (47.8%) | 131 (25.0%) | 220 (30.9%) | <0.001 |
| >30-60 mg/day | 67 (36.0%) | 50 (9.52%) | 117 (16.5%) | <0.001 |
| Azathioprine | 100 (51.8%) | 149 (25.1%) | 249 (31.7%) | <0.001 |
| Cyclophosphamide | 105 (54.4%) | 90 (15.2%) | 195 (24.8%) | <0.001 |
| Mofetil Mycophenolate | 79 (41.6%) | 83 (14.0%) | 162 (20.7%) | <0.001 |
| Igiv | 17 (8.90%) | 3 (0.514%) | 20 (2.58%) | <0.001 |
Conclusion Almost 25% of patients presented at least one hospitalization due to infection, being the respiratory infections the most frequent. Lower age al diagnosis, lower educational level, higher damage score, low complement, pericarditis, high esteroids doses and immunosuppressant increased the chance of having an admission due to serious infection. As well as the treatment with Igiv, an association that we can only explain by the reason that we only indicate it in severely active and infected patients.
Reference [1] Barber MRW, Clarke AE. Systemic lupus erythematosus and risk of infection. Expert Rev Clin Immunol. 2020 May;16(5):527-538. doi: 10.1080/1744666X.2020.1763793. Epub 2020 Jun 1. PMID: 32478627.
Acknowledgements To Karen Roberts who did the statical analysis and the UNISAR for the support.
Disclosure of Interests None Declared.
Keywords: Systemic lupus erythematosus, Infection-related RMDs
DOI: 10.1136/annrheumdis-2023-eular.1867