fetching data ... 
Background: Behçet’s Disease (BD); is characterized by oral and genital ulcers, arthritis, skin manifestations, uveitis, gastrointestinal tract and central nervous system involvement [1]. Although it is known to be more severe in men, there are studies in the literature with conflicting results regarding gender and the distribution of clinical findings.
Objectives: This study aimed to examine the relationship between clinical findings and gender in BD patients and to compare our results with the literature.
Methods: According to the classification criteria of the International Study Group, 506 patients diagnosed with Behçet’s disease were included in the study. Demographic data and laboratory and clinical findings of the patients were obtained retrospectively from hospital records, and the distribution of clinical findings by gender was evaluated.
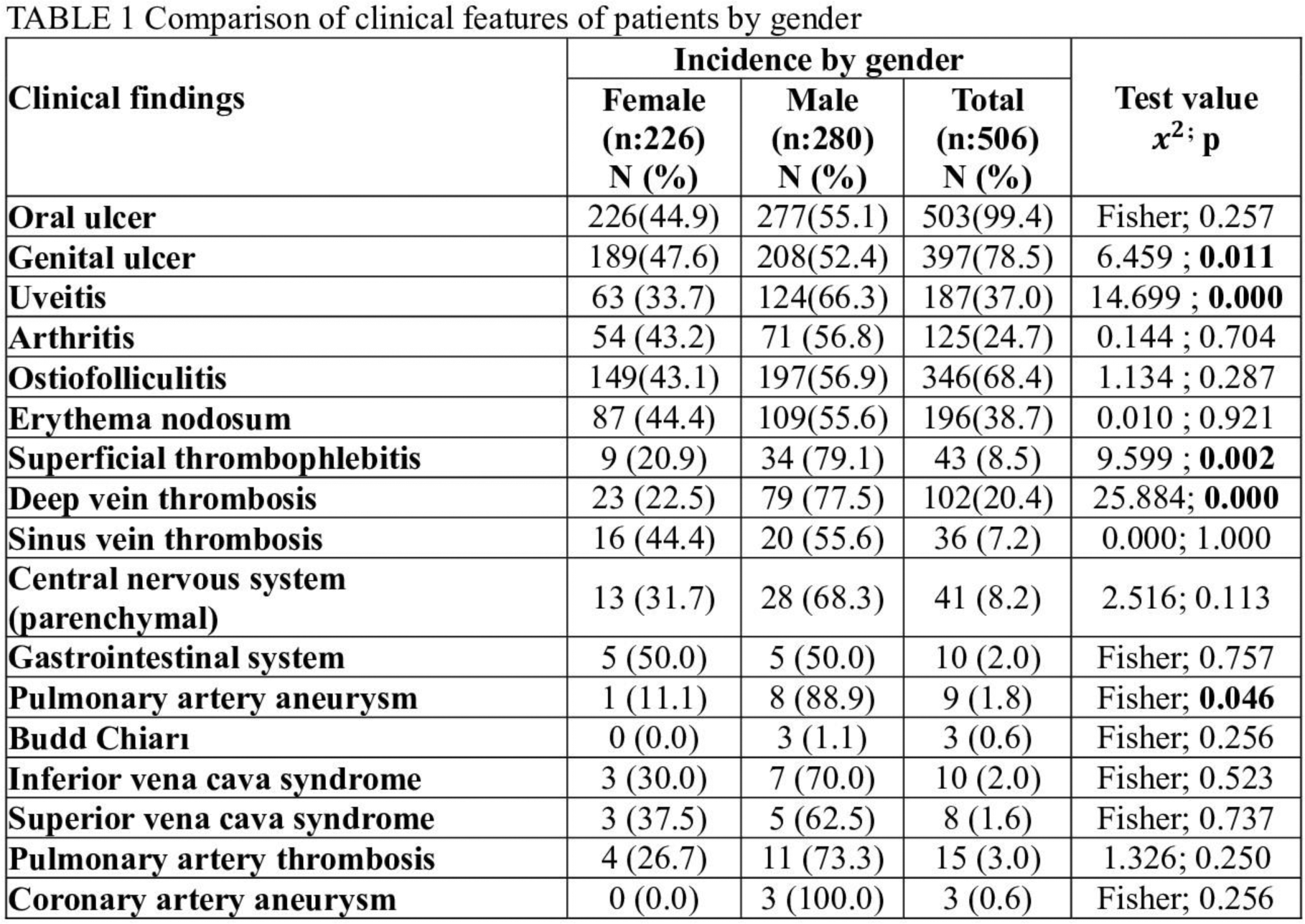
Results: A total of 280 males (55.3%) and 226 females (44.7%) were included in the study. The mean age at the beginning of symptoms was 23.00±10.23 years, and the mean age at diagnosis was 29.00±9.62 years. There was no significant difference between male and female patients in terms of age at diagnosis (p:0.662). Genital ulcer (47.6% vs 52.4%, p:0.011), superficial thrombophlebitis (20.9% vs 79.1%, p:0.002), uveitis (33.7% vs 66.3%, p:0.02), deep vein thrombosis (DVT) (22.5% vs 77.5%, p:0.00) and pulmonary artery aneurysm (PAA) (11.1% vs 88.9%, p:0.046) were more common in males. There was no significant difference between the sexes in other clinical findings (Table 1). The rate of smoking was higher in male patients than in females (p:0.00). Family history of oral ulcer and Behçet’s disease were similar in both sexes (p: 0.310 and p: 0.858, respectively). There was no difference between the sexes in HLA B5 and pathergy test positivity (p: 0.783 and p: 0.234, respectively).
Conclusion: BD is a multi-systemic vasculitis that occurs in young adults and gender may affect clinical findings. Similar to the literature, the male-female ratio was 1.23 in our study [2]. Genital ulcers, superficial thrombophlebitis, uveitis, DVT, and PAA were more common in male patients than in females, and the difference was statistically significant. Other forms of vascular involvement (Budd Chiari, vena cava superior and inferior syndrome, pulmonary thrombus and coronary artery aneurysm) were more common in men, but the difference was not statistically significant due to the low number of patients. Considering the effect of vascular involvement on mortality, it can be concluded that it is more severe in men. In the literature, there are also studies showing that genital ulcers and joint findings are at the forefront in women, and eye, skin, and vascular involvement are more common in men [3]. Although studies are showing that genetic risk is higher in men and genetic factors play a role in the different presentation of the disease, we could not show a relationship between gender and HLA B5 positivity in our patient population [4]. In conclusion, gender has an impact on the clinical manifestations of BD and should be considered in patient follow-up. However, it is a heterogeneous disease, other factors may certainly affect the emergence of clinical findings.
REFERENCES: [1] Yazici Y, Hatemi G, Bodaghi B et al (2021) Behçet syndrome. Nat Rev Dis Primers 7(1):67.
[2] Ugurlu N, Bozkurt S, Bacanli A, Akman-Karakaş A, Uzun S, Alpsoy E. The natural course and factors affecting severity of Behçet’s disease: a single-center cohort of 368 patients. Rheumatol Int. 2015; 35:2103–7.
[3] Bonitsis NG, Luong Nguyen LB, et al. Gender-specific differences in Adamantiades-Behçet’s disease manifestations: an analysis of the German registry and meta-analysis of data from the literature. Rheumatology (Oxford). 2015; 54(1):121-33.
[4] Jo YG, Ortiz-Fernández L, Coit P, et al. Sex-specific analysis in Behçet’s disease reveals higher genetic risk in male patients. J Autoimmun. 2022; 132:102882.
Acknowledgements: NIL.
Disclosure of Interests: None declared.